
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-149
Challenging Case of Single Access Impella Assisted Double Vessel Angioplasty
By Dr Naveen Bhamri
Presenter
Dr Naveen Bhamri
Authors
Dr Naveen Bhamri1
Affiliation
Max Super Speciality Hospital, India1,
View Study Report
TCTAP C-149
Coronary - Hemodynamic Support
Challenging Case of Single Access Impella Assisted Double Vessel Angioplasty
Dr Naveen Bhamri1
Max Super Speciality Hospital, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Pt Had H/O high grade fever with chills ,body ache increasing shortness of breath and neck pain from last three days BP-90/60PR-102/MinSPO2=99%RR-20/MinO/E-GC CRITICALChest-B/L air entry present PA-soft Non Tender CVS -S1S2ACS Trop positive severe LV Dysfunction -20-25%

Relevant Test Results Prior to Catheterization
focal calcified Aortic Valve Mild MRTraces ARSpontaneous ECHO contrast seen in LV
Relevant Catheterization Findings
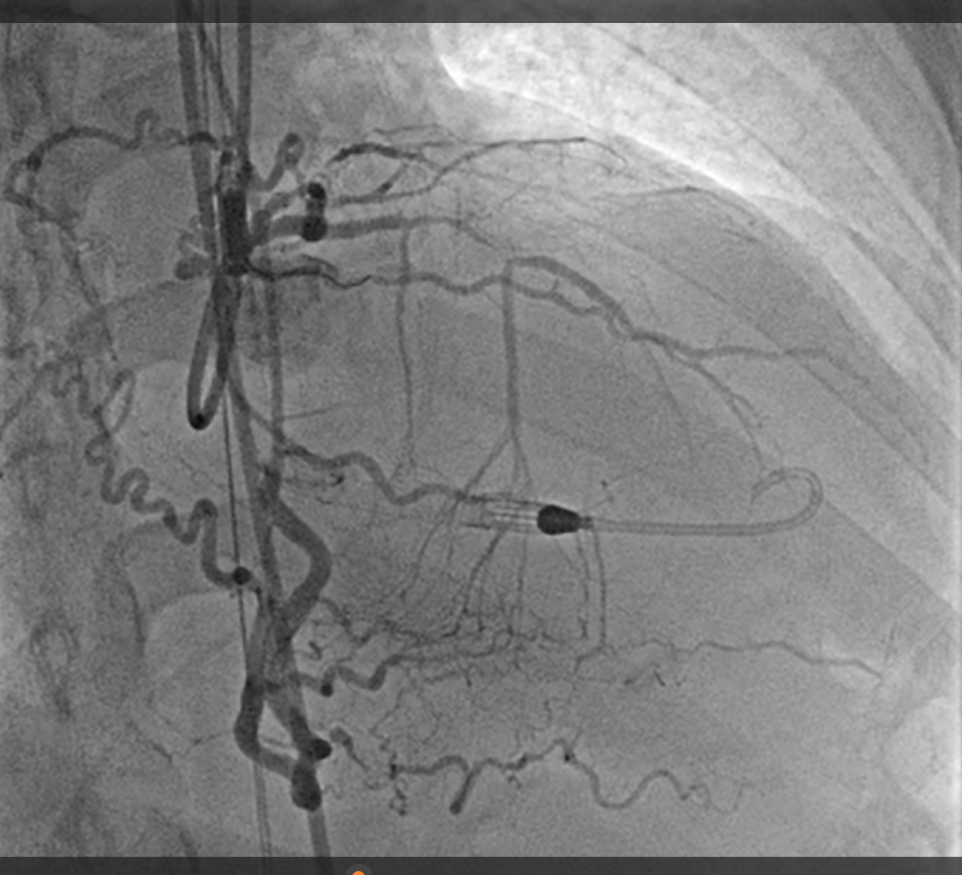
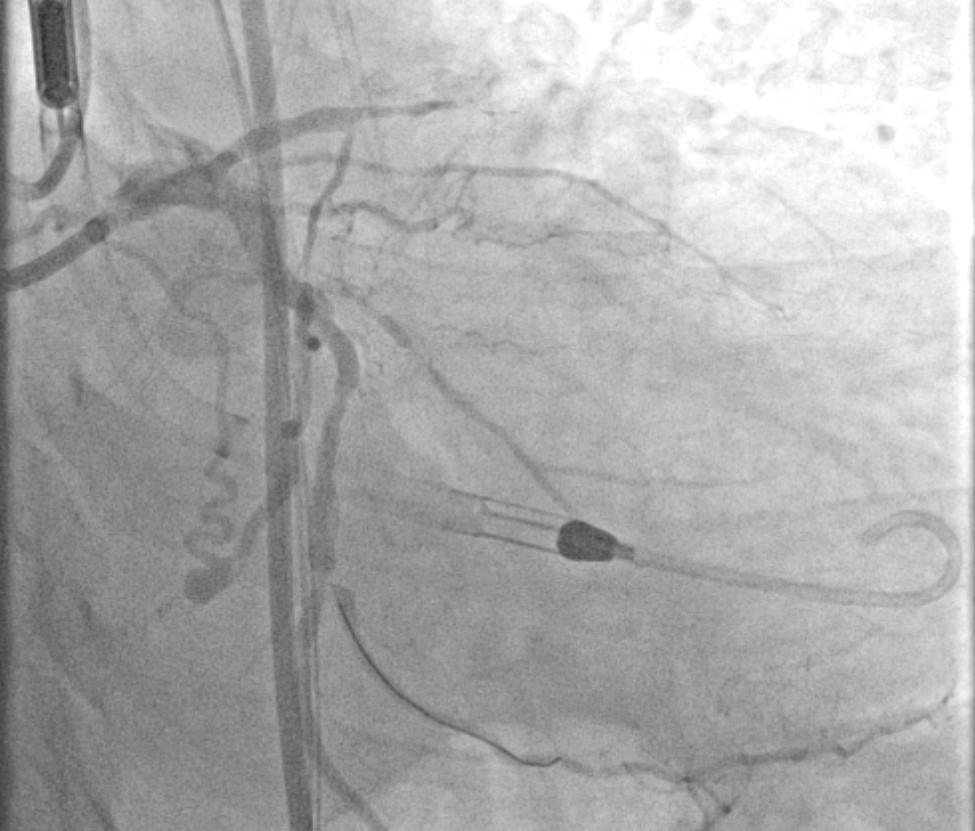
CAG Findings -Left Main Normal LAD-type 3 mid LAD 100% stenosis LCX-NON Dominant Prox LCX 90% ,tubular Conc stenosis OM1 ostial 99% tubular Conc stenosis,OM2 80% ,OM3 90% Tubular Conc stenosis 'RCA-Dominant Normal consent taken for high risk angioplasty (Impella assisted ,IVUS Guided ,PA pressure guided)

Interventional Management
Procedural Step
6F JR 3.5 through Right Radial access for retrograde injection Impella inserted through right femoral artery using 14F sheath and placed in LV 2perclose proglide 6FR sutures deployed at 10 O'clock and 2 O'clock positions.PA pressure catheter inserted through Right femoral vein 7FR femoral Sheath inserted throgh the impella sheath 7FR EBU Guide engage LCAWhisper ES GW Placed in OM2Pre dilatation done with 2x12 mm SC balloon @11 ATMDES 2.25x24mm is deployed in OM3 and post dilated with 2.25x12 mm NC balloon @12 atm optimised with IVUS.OM2 POBA done with 2x12 DEBOM1 wired with fielder XT -A wire using Fine cross Micro catheter ,DES 2.25x38mm deployed and optimised with IVUS.DES 3.5X38 mm synergy deployed in prox LCX and and optimised with IVUS Rinato wire crossed over to LAD and DES 2.5x38mm deployed in mid LAD
got TIMI 3 flow Post procedure PA sat -43%Pt cardiac output measured to be only 2.4 L /Mit was decided to keep Impella in Situ and start MILRINONE infusion wean off impella CP and maintain between 160-180impella was weaned off and removed ,Normal VALVE echos

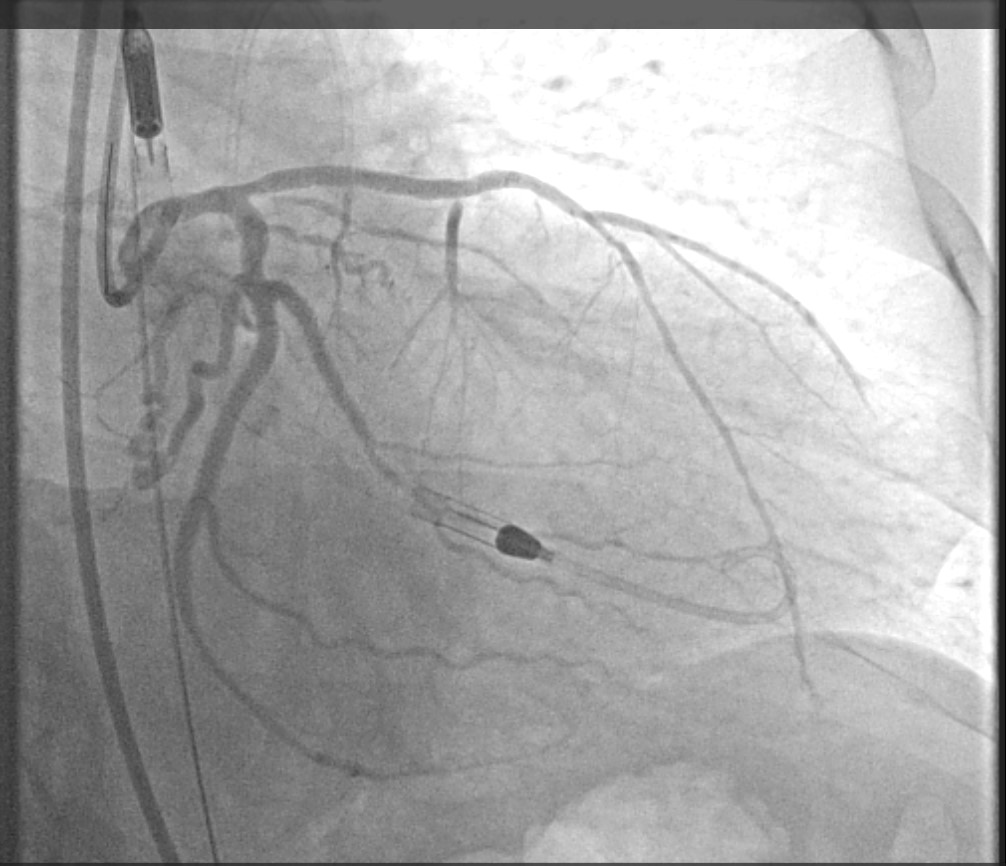
got TIMI 3 flow Post procedure PA sat -43%Pt cardiac output measured to be only 2.4 L /Mit was decided to keep Impella in Situ and start MILRINONE infusion wean off impella CP and maintain between 160-180impella was weaned off and removed ,Normal VALVE echos
Case Summary
a Single large bore 14FR access is a safe and effective option for performing complex pci in hemodynamically unstable pts with severe LV dysfunction ,care needs to be taken for a safe and careful puncture to avoid site complications. A technique using micro puncture needle with Ultrasound and flouro guidance. ensure safety of procedure AND must be utilize in every case .Contralateral small bore sheath can be used for angiography of femoral artery prior to puncture, this adds exrtra layer of security by ensuring central luminal punture.2 perclose proglide sutures deployed @10 & 2 oclock position .Using a swan Ganz catheter for monitoring PA pressures is helpful in pts with Ca