
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-046
A Challenging Case Report: A Case of Successful Device Delivery With Lesion Modification by ELCA
By Takeshi Sasaki, Taro Takeyama, Keisuke Nakabayashi, Nobuhito Kaneko, Hiroshi Ando
Presenter
Takeshi Sasaki
Authors
Takeshi Sasaki1, Taro Takeyama2, Keisuke Nakabayashi1, Nobuhito Kaneko1, Hiroshi Ando1
Affiliation
Kasukabe Chuo General Hospital, Japan1, Dokkyo Medical University Saitama Medical Center, Japan2,
View Study Report
TCTAP C-046
Coronary - Complex PCI - Calcified Lesion
A Challenging Case Report: A Case of Successful Device Delivery With Lesion Modification by ELCA
Takeshi Sasaki1, Taro Takeyama2, Keisuke Nakabayashi1, Nobuhito Kaneko1, Hiroshi Ando1
Kasukabe Chuo General Hospital, Japan1, Dokkyo Medical University Saitama Medical Center, Japan2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
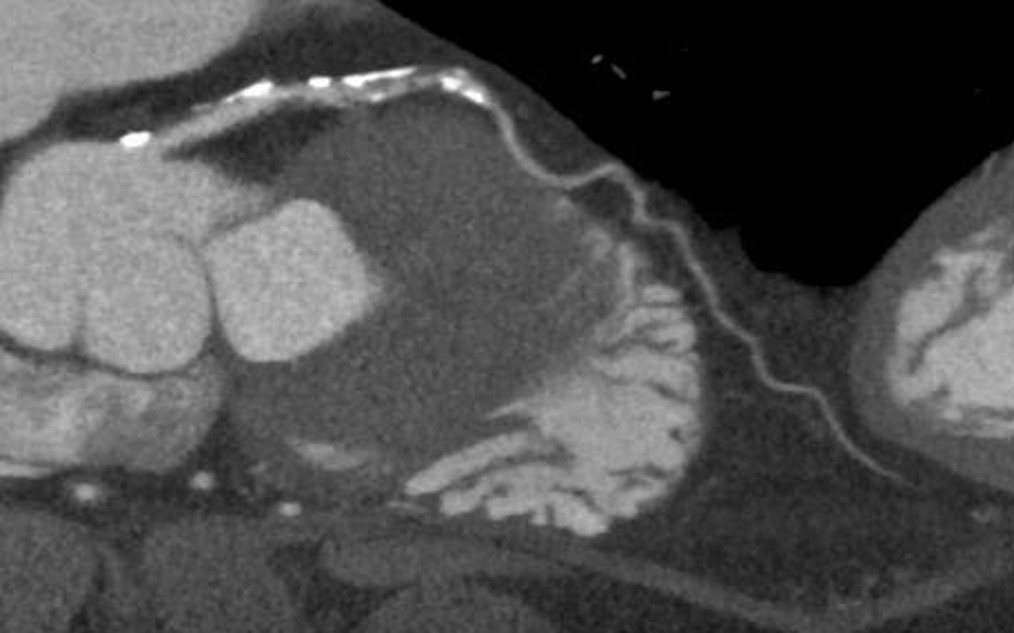
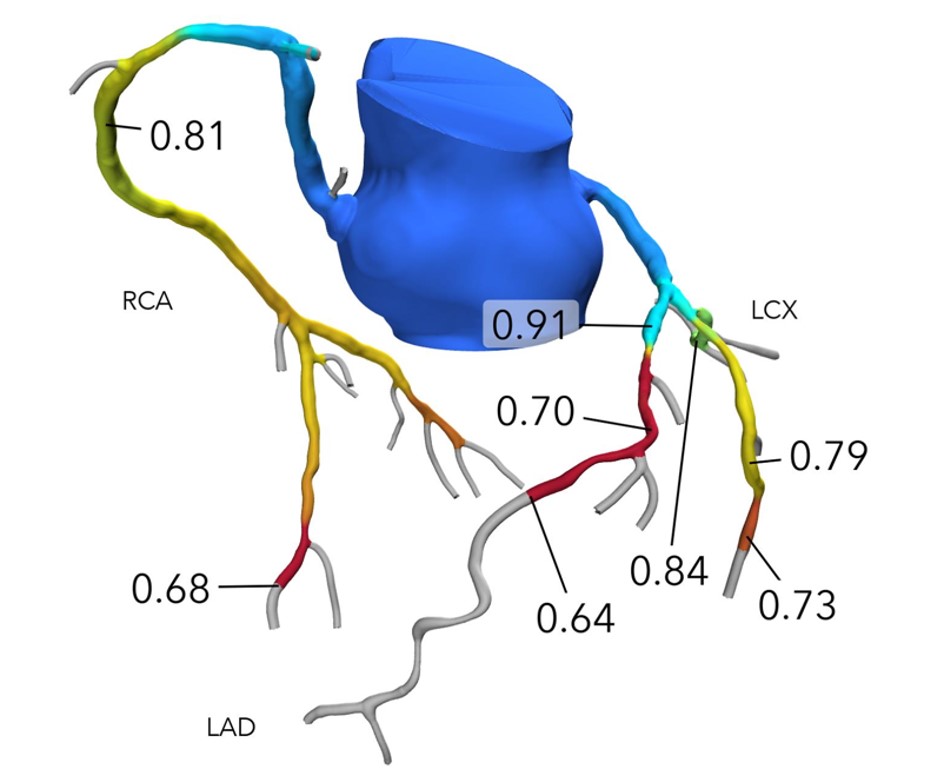
The patient who scheduled for EVAR for abdominalaortic aneurysm is a 88-year-old man with hyper tension, hyper lipemia, diabetesmellitus and chronic kidney disease. preoperative coronary CT showed aperivascular calcification and a low plaque in blood vessel. FFRCT taken priorto surgery showed significant stenosis (#6-7) of left anterior descendingartery (LAD).
Relevant Test Results Prior to Catheterization
Laboratory date: Creatinine 1.66mg/dL, LDL-cholesterol77mg/dL, Hemoglobin A1c 6.5%
Relevant Catheterization Findings
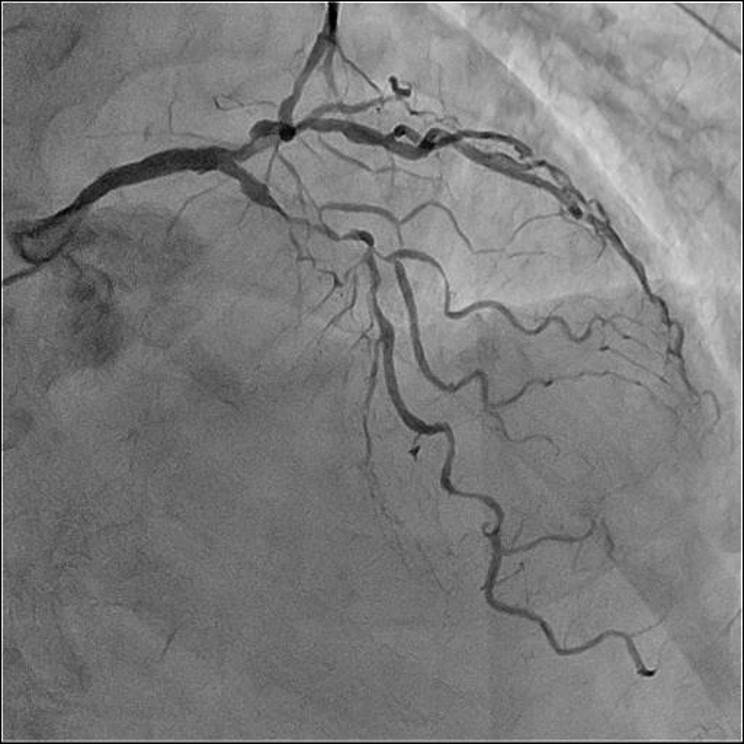
Initial angiography showed severe tortuousand calcified lesion in the middle LAD (#6-7).
Interventional Management
Procedural Step
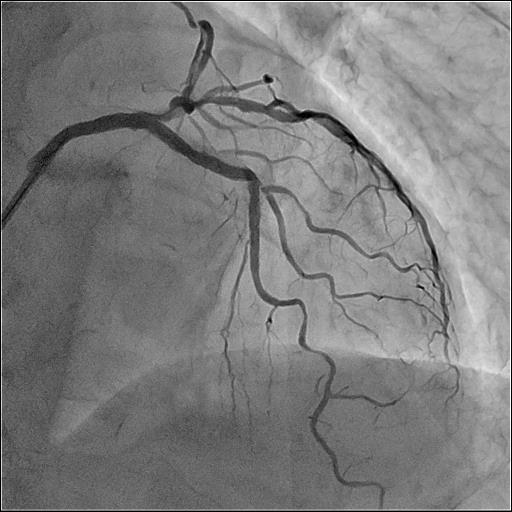
I engaged the left coronary artery with 7Fr-VL3.5from right radial artery. I crossed the SION blue guide-wire to diagonal branch(D2) and the SION to LAD with FINECROSS M. Intravascular ultrasound (IVUS) and Ryurei1.5*10mmfor anterior dilatation was not delivered. Angio showed severe tortus andcalcifid lesion. However, preoperative coronary CT showed a perivascularcalcification and a low plaque in blood vessel. I selected excimer laser (ELCA)as a debulking device. Because the target lesion was a severe tortuous and I consideredthe risk of complications such as vascular injury and distal embolization by selectingRota blator for low plaque lesions. Then, Ryurei was successfully delivered. Ievaluated IVUS and anteriorly dilated the lesions with Wolverine 2.0*10mm, Ryurei2.5*30mm and Sapphire NC24 3.0*15mm. I placed the two drug eluting stents(DES), Ultimaster Nagomi 2.5*28mm in #7 and Ultimaster Nagomi 3.0*24mm in #6. IVUSshowed poor expansion of stent proximal edge, so I posteriorly dilated withSapphireNC24 3.0*15mm. Finally, I confirmed good stent crimping with IVUS andgood flow with angio. I succeeded in the PCI.


Case Summary
In this case, the target lesion was severetortuous and angiographically calcified lesion. I considered the risk of complications suchas perforation and distal embolization by using Rota blator. For that reason, Iselected the ELCA.The mechanism of ELCA is decomposition of substances by lightirradiation and by vapor explosion. IVUS passed successfully by using ELCA. Ievaluated the lesion from IVUS and completed appropriate pci. ELCA could be one option if imaging devices such asIVUS does not pass.