
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-162
Angiography Derived 3D Physiologic Mapping of the Coronary Flow Using QFR for the Planning of the Complex PCI
By Oyunkhand Buyankhishig, Gereltuya Choijiljav, Damdinjav Enkhee, Bum-Erdene Batbayar, Surenjav Chimed, Batzaya Tsognemekh, Erdembileg Dandar, Khuyag Batmyagmar
Presenter
Oyunkhand Buyankhishig
Authors
Oyunkhand Buyankhishig1, Gereltuya Choijiljav1, Damdinjav Enkhee2, Bum-Erdene Batbayar2, Surenjav Chimed3, Batzaya Tsognemekh4, Erdembileg Dandar5, Khuyag Batmyagmar1
Affiliation
Intermed Hospital, Mongolia1, First State Central Hospital, Mongolia2, Third State Central Hospital, Mongolia3, National Cardiovascular Center In Mongolia, Mongolia4, Mongolian National University of Medical Sciences, Mongolia5,
View Study Report
TCTAP C-162
Coronary - Imaging & Physiology - FFR
Angiography Derived 3D Physiologic Mapping of the Coronary Flow Using QFR for the Planning of the Complex PCI
Oyunkhand Buyankhishig1, Gereltuya Choijiljav1, Damdinjav Enkhee2, Bum-Erdene Batbayar2, Surenjav Chimed3, Batzaya Tsognemekh4, Erdembileg Dandar5, Khuyag Batmyagmar1
Intermed Hospital, Mongolia1, First State Central Hospital, Mongolia2, Third State Central Hospital, Mongolia3, National Cardiovascular Center In Mongolia, Mongolia4, Mongolian National University of Medical Sciences, Mongolia5,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 62 old male patient who had persistent angina regardless of optimal medical treatment. Multiple cardiovascular risk factors including smoking, hypertension and hypercholesterolemia. Prior medications are anti-hypertensives andaspirin.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
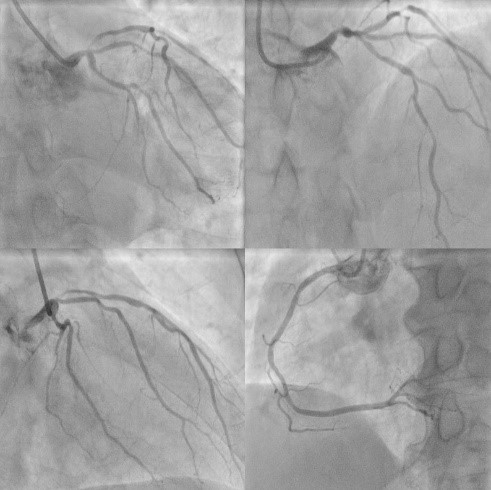
Diagnostic CAG showed diffuse lesions in LM and LAD including severe stenosis in distal LM and moderate stenosis in mid-LAD. LCx and RCA were normal and no significant stenosis.
Interventional Management
Procedural Step
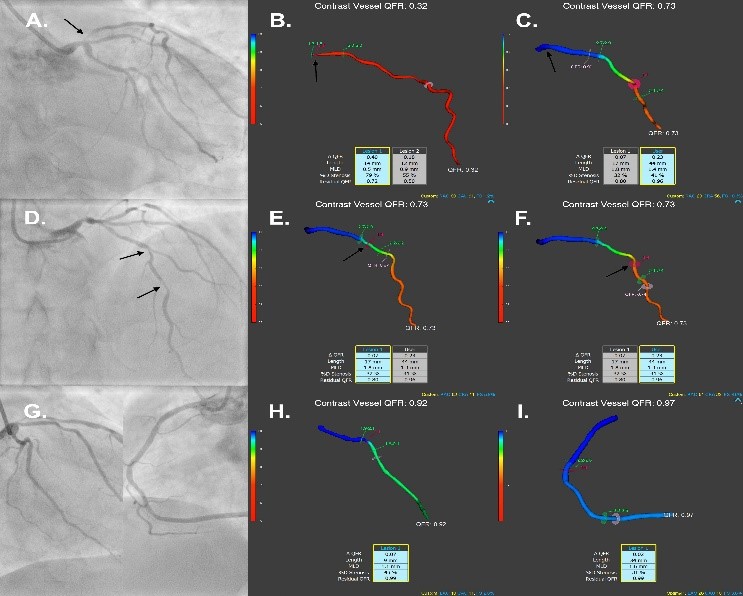
On diagnostic angiography, there was critical stenosis at the ostial LAD with the vessel QFR of 0.32 (arrow, Figure 1A and 1B). The proximal LAD lesion was successfully treated with drug-eluting stent (DES) which was implanted from LM to proximal LAD with final post-stenotic QFR of 0.99 (arrow, Figure 1C). There were another two isolated lesions (arrow, Figure 1D) with a total length of44mm in the mid LAD which have had post-stenotic QFR of 0.87 and 0.74, respectively (arrow, Figure 1E and 1F). The mid LAD lesions were untreated at the moment because vessel , and the patient was left on optimal medical treatment. Staged PCI could be considered for mid LAD lesions if the patient is symptomatic despite optimal medical treatment. The left circumflex (LCx) and right coronary artery (RCA) were normal (Figure 1G, 1Hand1I).
Case Summary
The angiography image-based3D-physiologic mapping of coronary physiology using the QFR could be a cost effective and non-invasive alternative to pressure wire based invasive approaches to guide complex PCI.