
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-171
What You See Is Not What You Imagine ; A Conundrum in Intervention
By Vijayendran Rajalingam, Faizal Khan Bin Abdullah, Glendon Seng Lau, Thurston Erng, Asri Ranga, Kamaraj Selvaraj, Abd Kahar Abd Ghapar
Presenter
Vijayendran Rajalingam
Authors
Vijayendran Rajalingam1, Faizal Khan Bin Abdullah1, Glendon Seng Lau2, Thurston Erng3, Asri Ranga1, Kamaraj Selvaraj1, Abd Kahar Abd Ghapar1
Affiliation
Sultan Idris Shah Serdang Hospital, Malaysia1, Hospital Sultan Idris Shah Serdang, Malaysia2, Serdang Heart Centre, Malaysia3,
View Study Report
TCTAP C-171
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
What You See Is Not What You Imagine ; A Conundrum in Intervention
Vijayendran Rajalingam1, Faizal Khan Bin Abdullah1, Glendon Seng Lau2, Thurston Erng3, Asri Ranga1, Kamaraj Selvaraj1, Abd Kahar Abd Ghapar1
Sultan Idris Shah Serdang Hospital, Malaysia1, Hospital Sultan Idris Shah Serdang, Malaysia2, Serdang Heart Centre, Malaysia3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A Case of 56 year old Male had a history of Acute Anterior Myocardial Infarction 6 months ago . He presented to a Non Cardiac Hospital was given thrombolysis and subsequent dual anti-platlets and high dose statin . He remained Anginal Free and was able to carry out routine activity as usual. Clinically well Built Bp 110/80 mmhg PR 80 bpm .He was then referred to us for Angiogram as outpatient.
Relevant Test Results Prior to Catheterization
Echocardiography : Anterior Wall Hypokinetic with preserved Ejection Fraction (55% )
Fasting Lipid : TCH 6 / HDL 1.4 / LDL 3.6 / TG 2.6Renal Profile : Ur 9 K 4.2 Na 140 Creatinine 95 Full Blood Count : Hb 12 WCC 5 Platelet 210 HCT 40
Fasting Lipid : TCH 6 / HDL 1.4 / LDL 3.6 / TG 2.6Renal Profile : Ur 9 K 4.2 Na 140 Creatinine 95 Full Blood Count : Hb 12 WCC 5 Platelet 210 HCT 40
Relevant Catheterization Findings
Right Dominant System

Right Coronary Minor Irregularities
Left System
mid- LAD stenosis 50 - 60% stenosis with an Ulcerated Plaque seen from Angiogram
LCX minimal stenosis mid LCX 20-30%
Left Main smooth
Interventional Management
Procedural Step
As the Angiogram findings shows a vulnerable plaque with TIMI 3 flow and patient is asymptomatic ,questions arise if there is a need to defer stenting and continue with Optimal Medical Therapy .However in view that patient had a History of Myocardial Infarction and Echocardiography showed Anterior Septal Hypokinesia we decided to proceed with Coronary Imaging for optimal decision .
Engaged Left System with EBU 3.5 6fr then wired with Sion Blue gw. Immediately proceed with Optical Coherance Tomography (OCT) run without predilating to assess the originality of the plaque characteristics MLD ( morphology . length , diameter ) from the OCT able to demonstrate an Ulcerated dissecting plaque with MLA of 2.1 at mid LAD . Hence we decided to Intervene the lesion by predilating with Non Compliant Balloon 3.5 x 15 and proceeded to stent with DES 3.5 X 32mm and we further post dilate with a Non Compliant Balloon 4.0 x 15mm Before repeating final OCT run again ensuring stent is well apposed , well expanded and no Distal Stent Edge Dissection ( MAX )

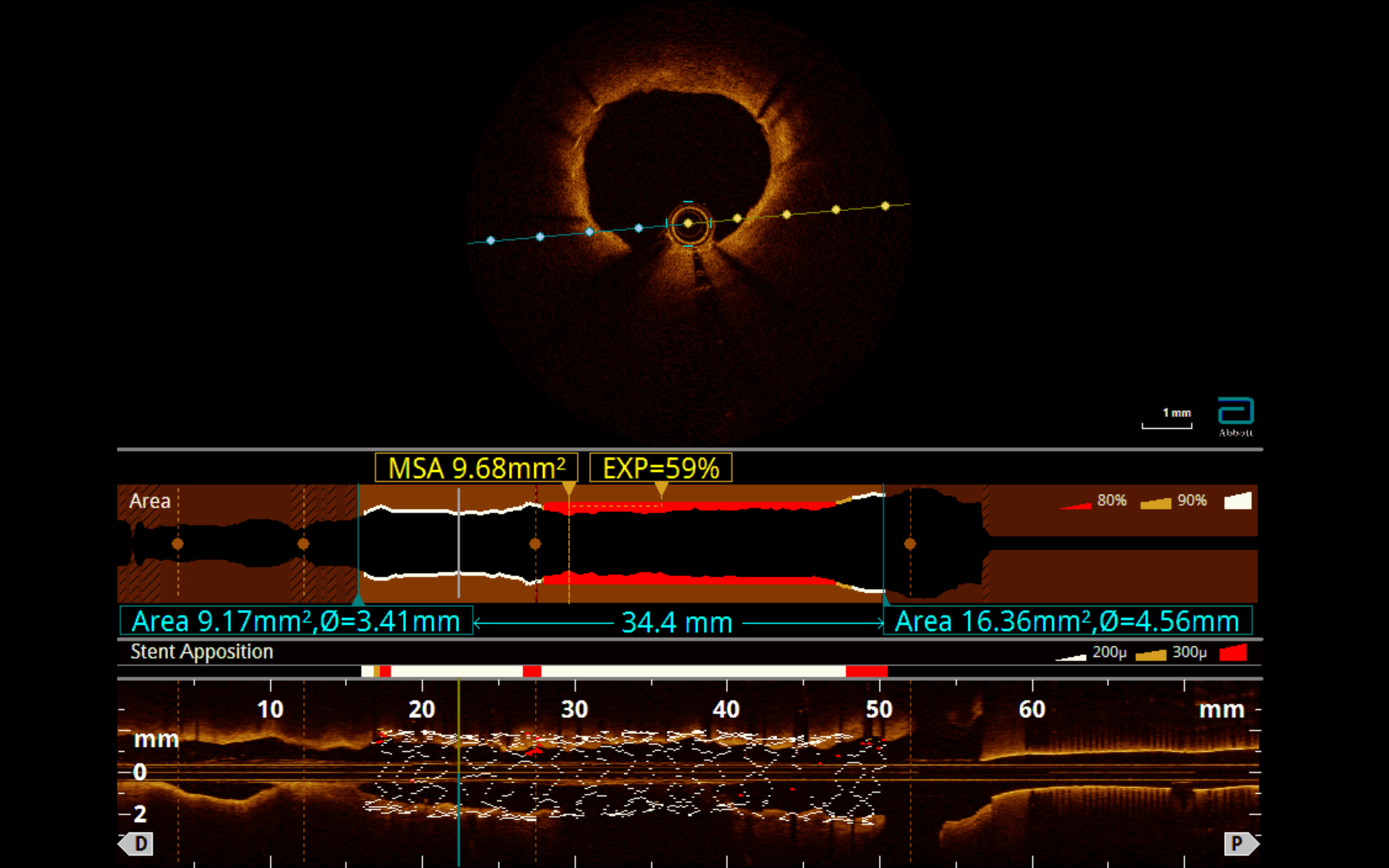
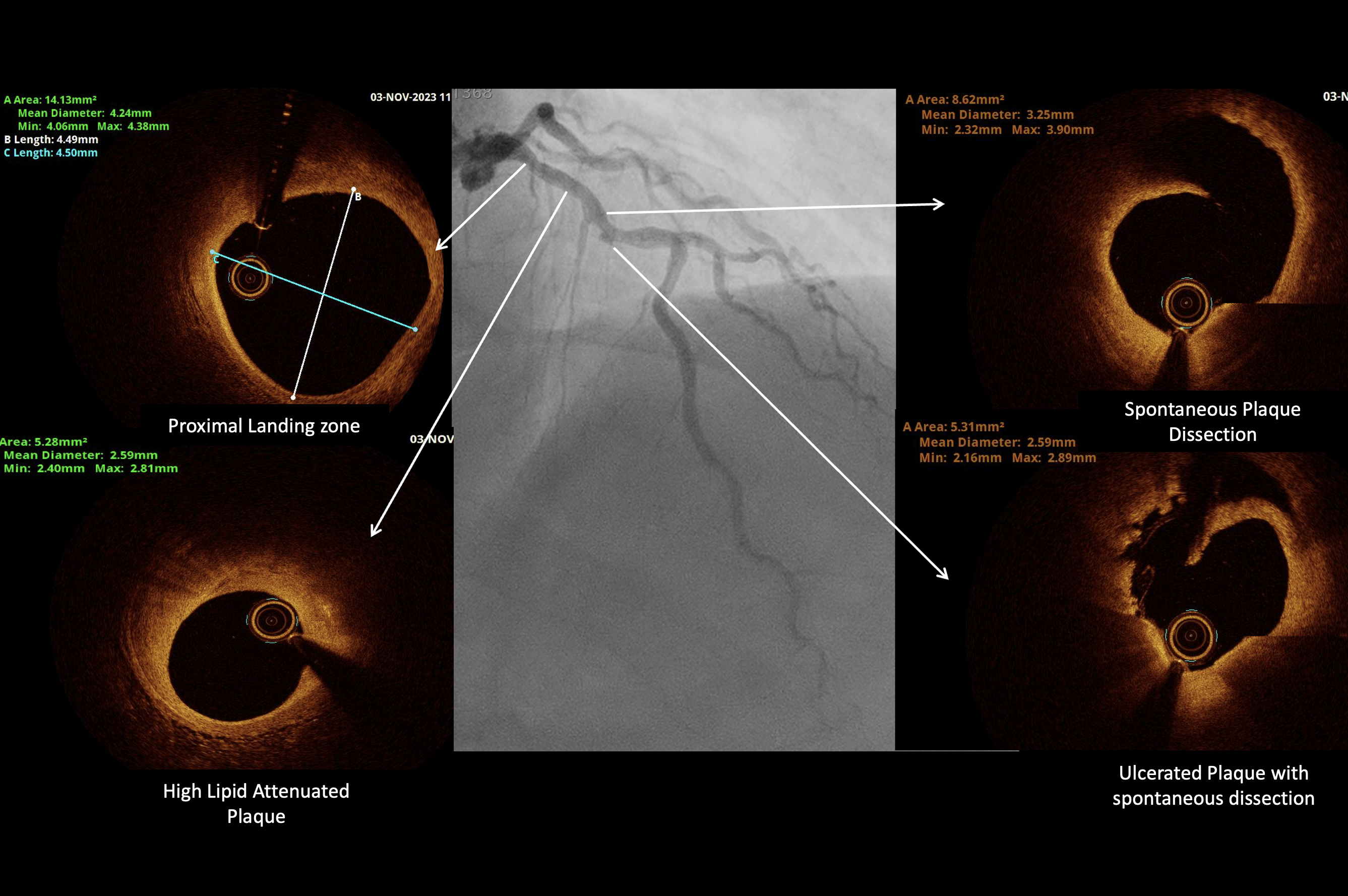
Engaged Left System with EBU 3.5 6fr then wired with Sion Blue gw. Immediately proceed with Optical Coherance Tomography (OCT) run without predilating to assess the originality of the plaque characteristics MLD ( morphology . length , diameter ) from the OCT able to demonstrate an Ulcerated dissecting plaque with MLA of 2.1 at mid LAD . Hence we decided to Intervene the lesion by predilating with Non Compliant Balloon 3.5 x 15 and proceeded to stent with DES 3.5 X 32mm and we further post dilate with a Non Compliant Balloon 4.0 x 15mm Before repeating final OCT run again ensuring stent is well apposed , well expanded and no Distal Stent Edge Dissection ( MAX )
Case Summary
It may seem moderate Lesion angiographically , with Imaging ( OCT ) we were able to demonstrate an Unstable Vulnerable Plaque with tight Lumen ( MLA 2.1 ) .Would it be fair and save to defer stenting in such vulnerable plaque or should we use Functional Testing ( FFR /RFR) or Minimal lumen Area ( MLA ) from Imaging to decide as patient is asymptomatic. There is ongoing discussion on treatment of vulnerable in asymptomatic patients Usage of Imaging is a game changer allows us to make decision intervening a particular lesion : Morphology , Length , Diameter ( MLD) and Post Stent assessment Medial dissection , Apposition , Expansion ( MAX)