
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-172
OCT- A Friend With Benefit
By Fazila Malik, Nazmun Laila
Presenter
Nazmun Laila
Authors
Fazila Malik1, Nazmun Laila1
Affiliation
National Heart Foundation Hospital & Research Institute, Bangladesh1,
View Study Report
TCTAP C-172
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
OCT- A Friend With Benefit
Fazila Malik1, Nazmun Laila1
National Heart Foundation Hospital & Research Institute, Bangladesh1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
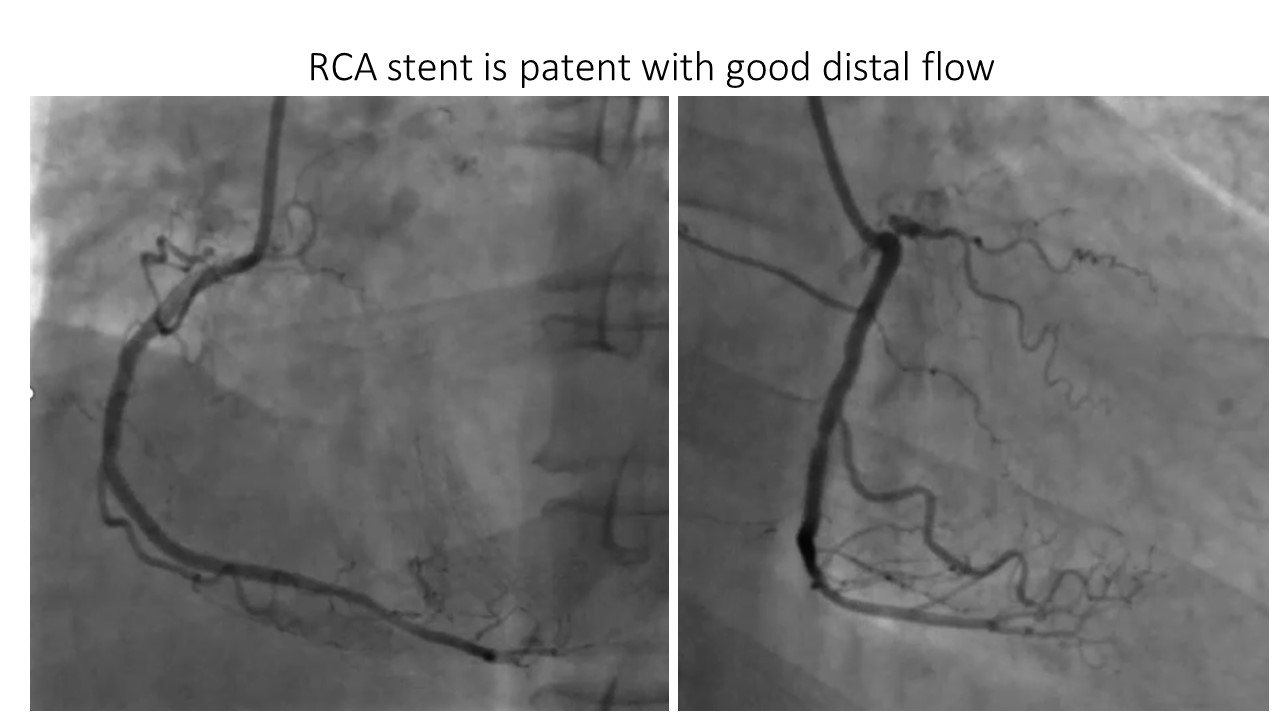
A 50-year-old gentleman presented with typical anginal chest pain for the past 2 days. He is previously hypertensive,non diabetic and had no family history of coronary artery disease. He had a history of PCI to RCA in 2021 (CTO). He was hemodynamically stable , with a blood pressure of 110/70 mmHg and heart rate of 92 bpm.
Relevant Test Results Prior to Catheterization
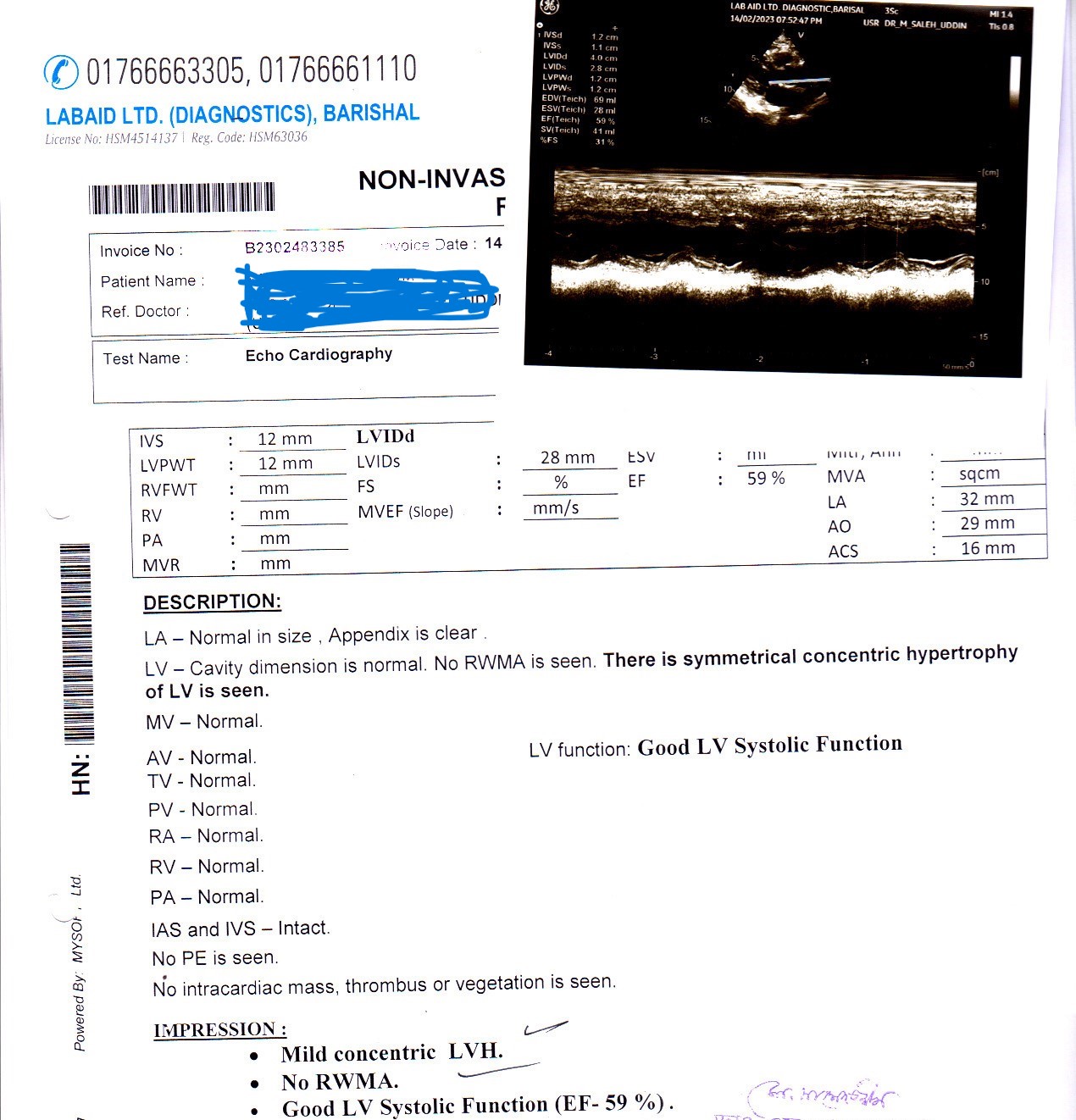
He had a borderline rise in troponin I (0.55 ng/dl) and echocardiography revealed preserved LV systolic function.

Relevant Catheterization Findings
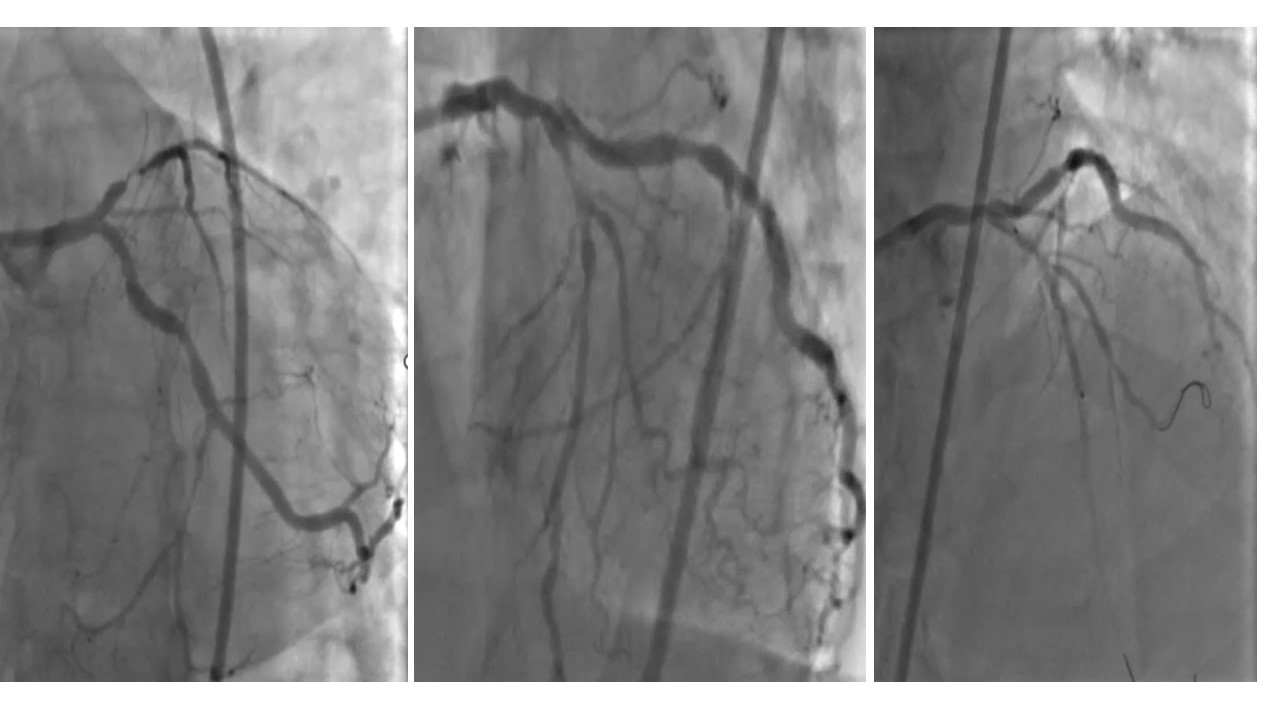
On Coronary angiogram, her RCA stent was found to be patent .LM had plaque burden in distal segment involving bifurcation of both LAD and LCX. LAD had a 90-95% stenosis involving the origin of first Diagonal. LCX was diffusely diseased in its distal part.

Interventional Management
Procedural Step
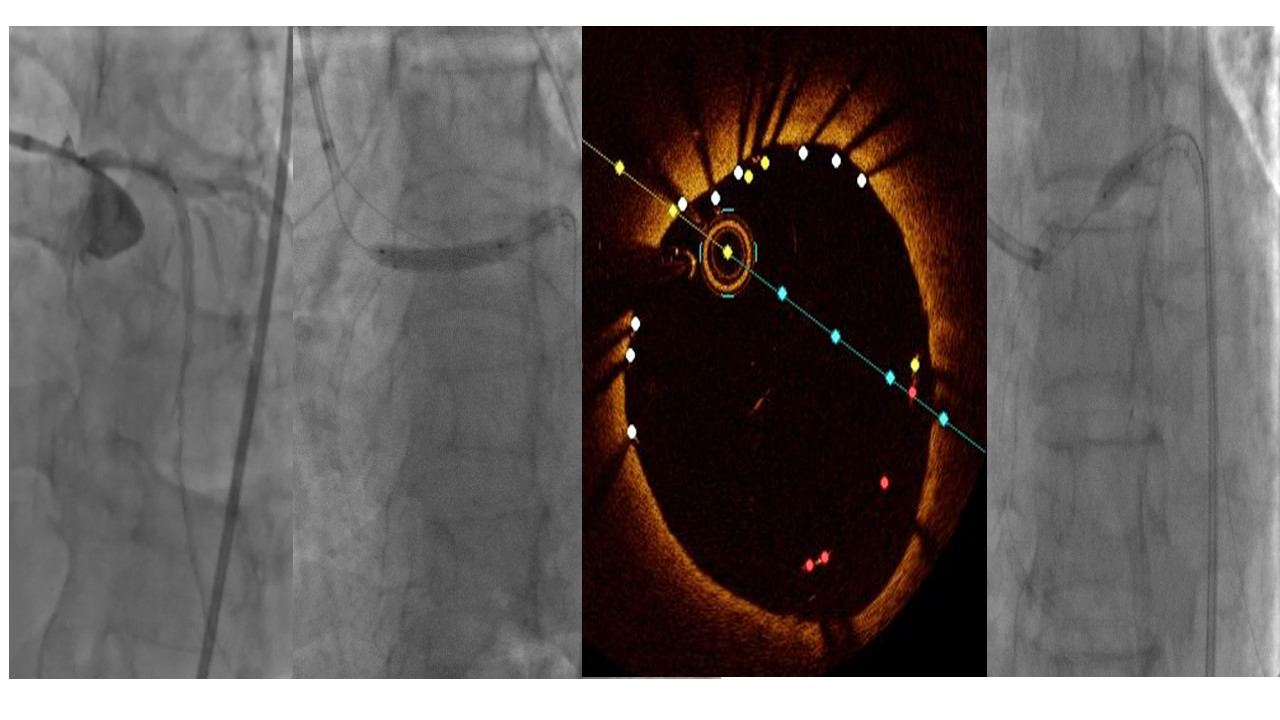
Both LAD and LCX were wired, LAD was predilated with a 2.0 x 15mm balloon. An OCT run revealed that the distal landing zone was markedly small in diameter in comparison to the proximal landing zone in LM. At LM Bifurcation it is Medina 1,1,0 with LCX origin free of significant disease. At LAD, D1 level, the score is
Medina 1,1,1, with severe stenosis involving the diagonal vessel. So the LCX wire was manoeuvred into First Diagonal and diagonal was dilated gently with a
2.0 x 15 mm NC balloon. Due to differences in the lumen size proximally and distally, a 2.75 x 30mm DES was first deployed over the mid LAD lesion and a 3.5 x 24mm DES was deployed at 12 ATM proximally covering the LM lesion. This was followed by a POT using a 4.0 x 8mm NC balloon. Post stent OCT revealed a well
apposed LAD stent with good stent strut expansion and no distal dissection. At LM bifurcation LCX ostia is free, but there was gross mal- apposition of the
proximal edge of LM stent at 3 o’clock to 6 o’clock position ,evident from the red dots. A repeat POT was done with a 5.0 x 6mm NC balloon at 14 ATM. A final
OCT run showed a LM luminal area of 20.42mm2, well apposed stent struts with no dissections.

Case Summary
OCT is a very good imaging modality for pre-PCI and post PCI assessment. It gives a greater definition on lumen boundaries allowing for a more accurate calculation of lumen area. It also allows better assessment of stent expansion and apposition to the intima.