
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-185
Relative Merits of IVUS vs OCT in LM PCI- A Comparison
By Rohit Mody
Presenter
Rohit Mody
Authors
Rohit Mody1
Affiliation
Mody Harvard Cardiac Institute & Research Centre, India1,
View Study Report
TCTAP C-185
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
Relative Merits of IVUS vs OCT in LM PCI- A Comparison
Rohit Mody1
Mody Harvard Cardiac Institute & Research Centre, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Patient details- A patient who is 74 year old female with Angina on Exertion 3 (AOE 3), Dyspnea on Exertion 3 (DOE 3), Left Ventricular (LV) dysfunction, and Ejection fraction (EF) 25%, Normal Body mass index, restlessness, chest pain Angiography revealed Left Main (LM) with Double Vessel Disease (DVD) with Right Coronary Artery (RCA) normal
Relevant Test Results Prior to Catheterization
Prior tests- Diabetic Hypertensive AOE 3 DOE 3 LV Dysfunction EF 25% Obese Chronic Obstructive Pulmonary Disease (COPD)
Relevant Catheterization Findings
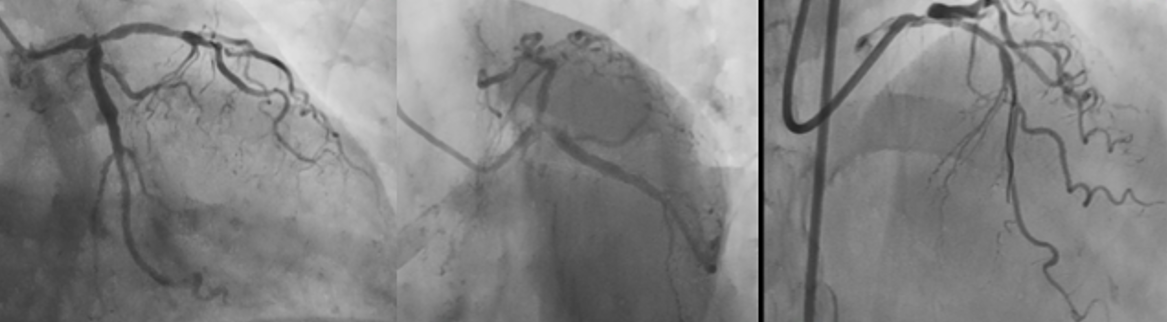
Angiography reveals- Left Main with Double Vessel Disease- DVD, RCA normal
Interventional Management
Procedural Step
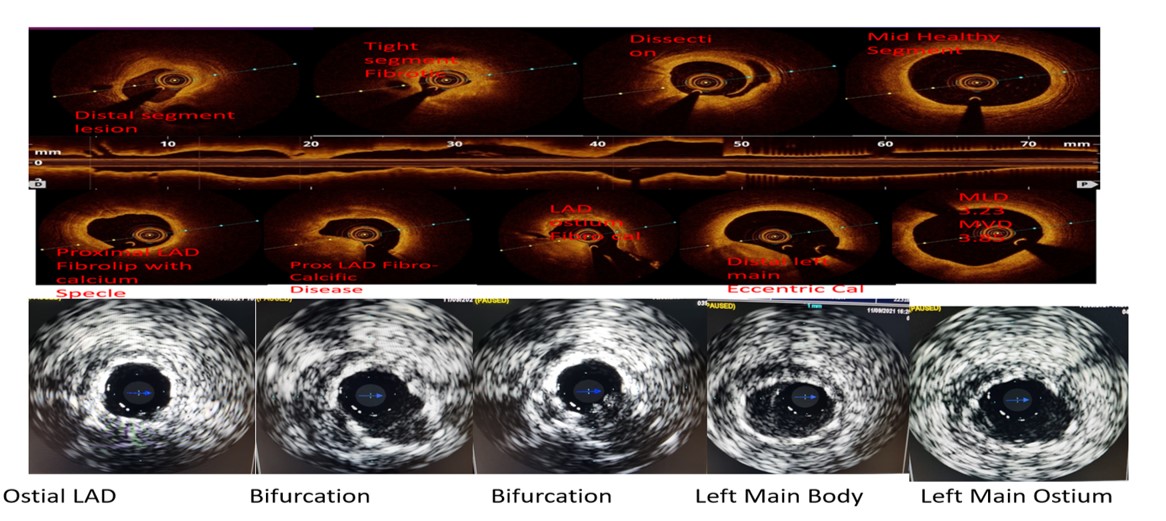
Angiography revealed DVD with RCA normal, LM hooked with EBU 7f, Intravascular Ultrasound (IVUS) & Optical Coherence Tomography (OCT) done to examine the anatomy and strategized.OCT Findings-OCT run taken with 10ml contrast injection for distal LAD to LM, Distal LAD ref. diameter 2.5mm, Proximal LAD ref. diameter 3.5mm, Lesion length- 55mm, LM distal 4.5mm, LM MLA achieve 4mm2 and LAD ostial- 3mm2
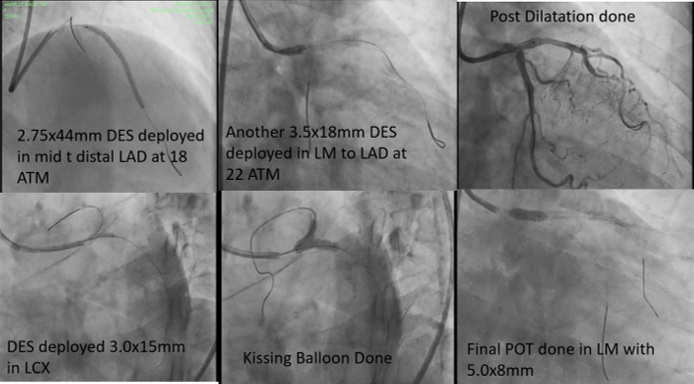
Then 2.75x44mm DES deployed in mid to distal LAD at 18 ATM, Another 3.5x18mm (Resolute Onyx- Zotarolimus Eluting Stent) DES deployed in LM to LAD at 22 ATM, Post Dilatation done using 3x12mm balloon, DES deployed 3.0x15mm (Resolute Onyx- Zotarolimus Eluting Stent) in LCX at 16 ATM, Kissing Balloon Done by keeping a 3.0x12 mm balloon in LAD & 3.0x10mm, Final POT done in LM with 5.0x8mm Balloon sparing Carina, Good final result, TIMI 3 flow achieved & no complications


Then 2.75x44mm DES deployed in mid to distal LAD at 18 ATM, Another 3.5x18mm (Resolute Onyx- Zotarolimus Eluting Stent) DES deployed in LM to LAD at 22 ATM, Post Dilatation done using 3x12mm balloon, DES deployed 3.0x15mm (Resolute Onyx- Zotarolimus Eluting Stent) in LCX at 16 ATM, Kissing Balloon Done by keeping a 3.0x12 mm balloon in LAD & 3.0x10mm, Final POT done in LM with 5.0x8mm Balloon sparing Carina, Good final result, TIMI 3 flow achieved & no complications
Case Summary
In LM PCI Imaging changes the decisions quite often and should always be encouraged in patients of especially this subset If we compare OCT with IVUS imaging the following points are noted- A. The Bifurcation of LM into LAD & LCX is more clearly visible with OCT and a decision to use either One-stent or two-stent strategy can be taken before hand B. The Calcium depth and extent is more clearly visible on OCT than IVUS C. The ostium is only visible with IVUS D. Optimization criteria are more well studied with IVUS than OCT Hence to conclude in LM PCI imaging with both OCT & IVUS can be complimentary to each other in decision Making