
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-111
Nightmare in Cathlab
By Hitendra M Bhagwatkar
Presenter
Hitendra M Bhagwatkar
Authors
Hitendra M Bhagwatkar1
Affiliation
NKPSIMS & RC, Lata Mangeshkar Hospital, Nagpur, India1,
View Study Report
TCTAP C-111
Coronary - Complication Management
Nightmare in Cathlab
Hitendra M Bhagwatkar1
NKPSIMS & RC, Lata Mangeshkar Hospital, Nagpur, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
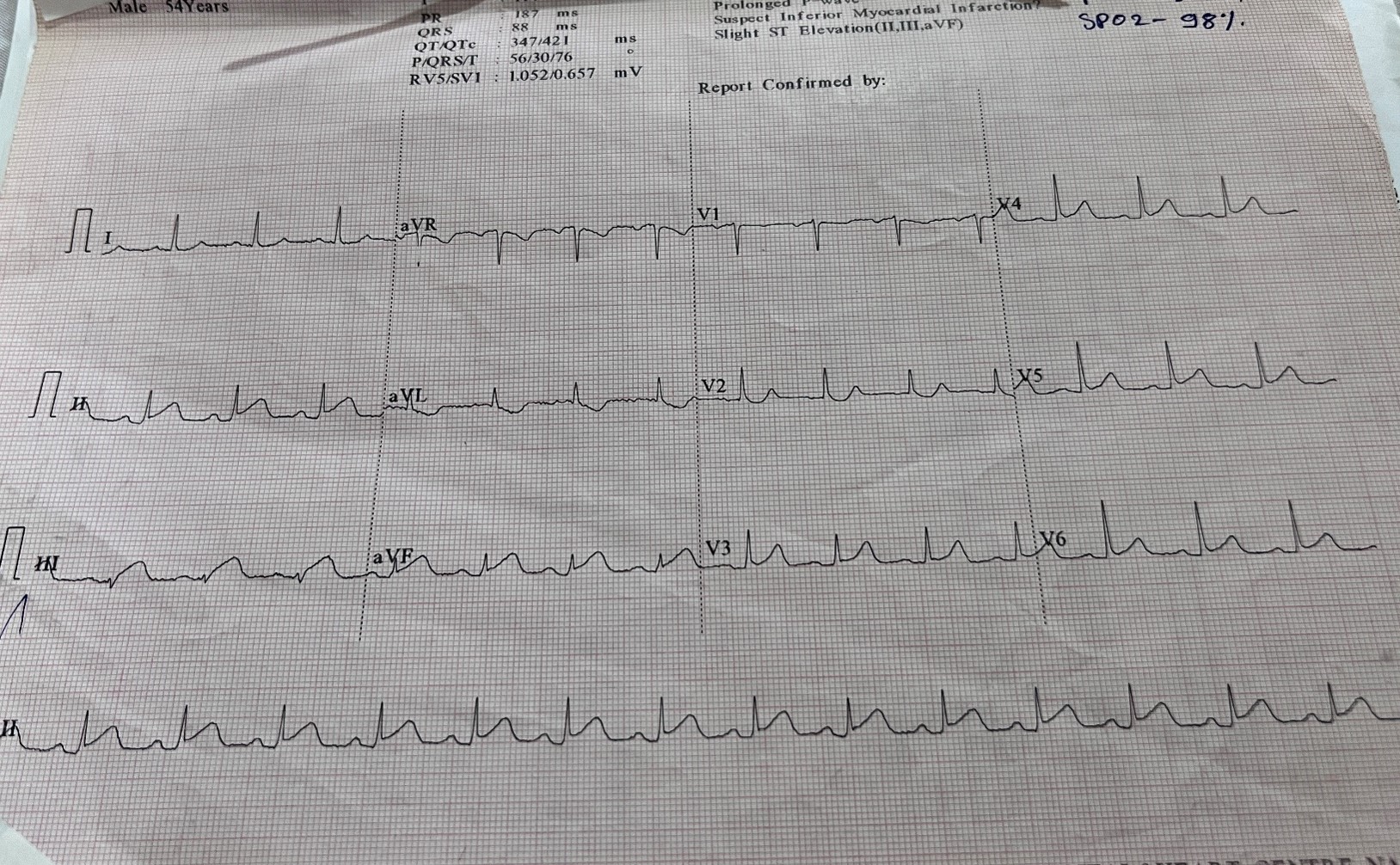
65 year old male admitted with Inferior wall MI
Relevant Test Results Prior to Catheterization
ECG –SHOWED IMWI
Relevant Catheterization Findings
CAG –showed TVD(Triple Vessel Disease)
RCA- Ectatic RCA ,proximal critical 90 % lesion
LAD –PROXIMAL 70%LESION
LCX- MID 80 %LESION

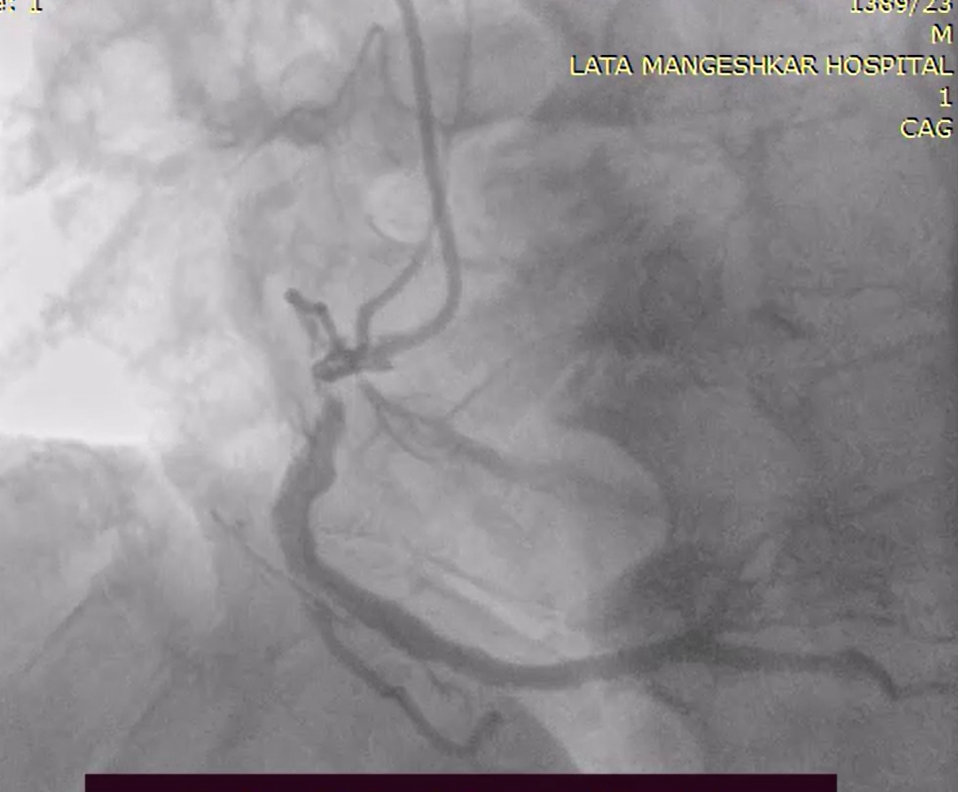
RCA- Ectatic RCA ,proximal critical 90 % lesion
LAD –PROXIMAL 70%LESION
LCX- MID 80 %LESION
Interventional Management
Procedural Step
RCA was engaged with JR 3.5 , 6 F , when we attempted to cross the wire workhorse hard wire Proximal RCA got dissected slow flow occurred
Finally was able to cross the wire through true lumen bypassing the dissected part of RCA . Attempted to cross 3.5 * 24 mm DES , but the stent could not cross the lesion and the whole symmetry got out and the catheter got disengaged. Trying to re engage the JR catheter , the ostioproximal RCA got dissected and there was slow flow in RCA, patient went into Complete Heart Block , temporary Pacemaker was Inserted. , Patient developed Re infarct with ECG showing fresh ST elevation in Inferior leads, developed Shock and inotrops accelerated.Final shoot showed complete dissection from ostial RCA to mid RCA with slow flow

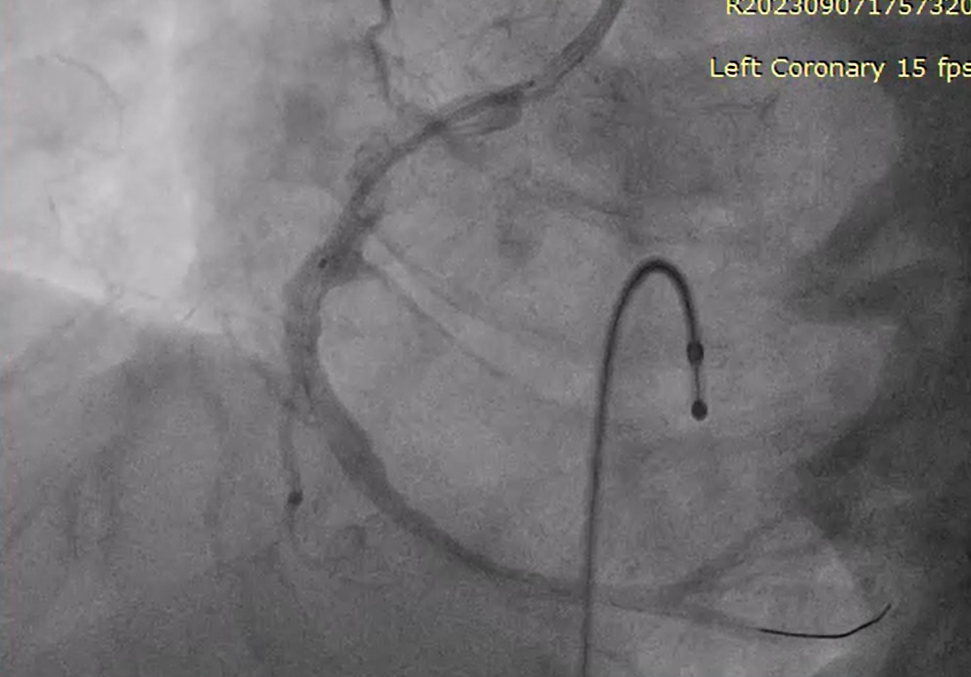

Finally was able to cross the wire through true lumen bypassing the dissected part of RCA . Attempted to cross 3.5 * 24 mm DES , but the stent could not cross the lesion and the whole symmetry got out and the catheter got disengaged. Trying to re engage the JR catheter , the ostioproximal RCA got dissected and there was slow flow in RCA, patient went into Complete Heart Block , temporary Pacemaker was Inserted. , Patient developed Re infarct with ECG showing fresh ST elevation in Inferior leads, developed Shock and inotrops accelerated.Final shoot showed complete dissection from ostial RCA to mid RCA with slow flow
Case Summary
Proper shoot in all angles is must for the assessment of lesion and tortuosity of vessel. Right selection of PTCA Guide wire preferably soft wire should be used To avoid dissection.Temporary Pacemaker should be placed before starting angioplasty procedure.Use of extra support like buddy wire or Guide liner is a must during stent implantation in torturous lesions. Cardiothoracic Surgery backup is a must in such cases.