
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-131
Successful Deployment of a Dislodged Stent With a Small Balloon Technique: Special Reference to Over the Wire System.
By Satej Sadashiv Janorkar
Presenter
Satej Janorkar
Authors
Satej Sadashiv Janorkar1
Affiliation
Deenanath Mangeshkar Hospital & Research Center, India1,
View Study Report
TCTAP C-131
Coronary - Complication Management
Successful Deployment of a Dislodged Stent With a Small Balloon Technique: Special Reference to Over the Wire System.
Satej Sadashiv Janorkar1
Deenanath Mangeshkar Hospital & Research Center, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
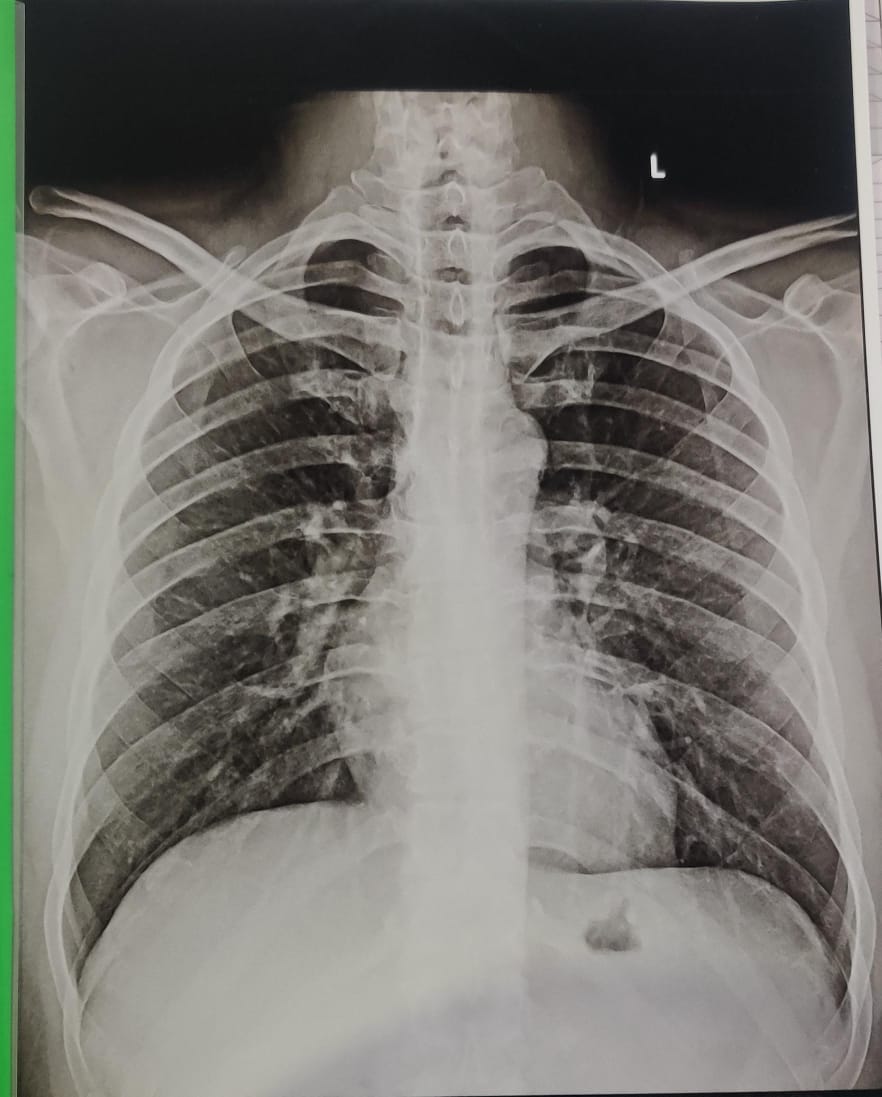
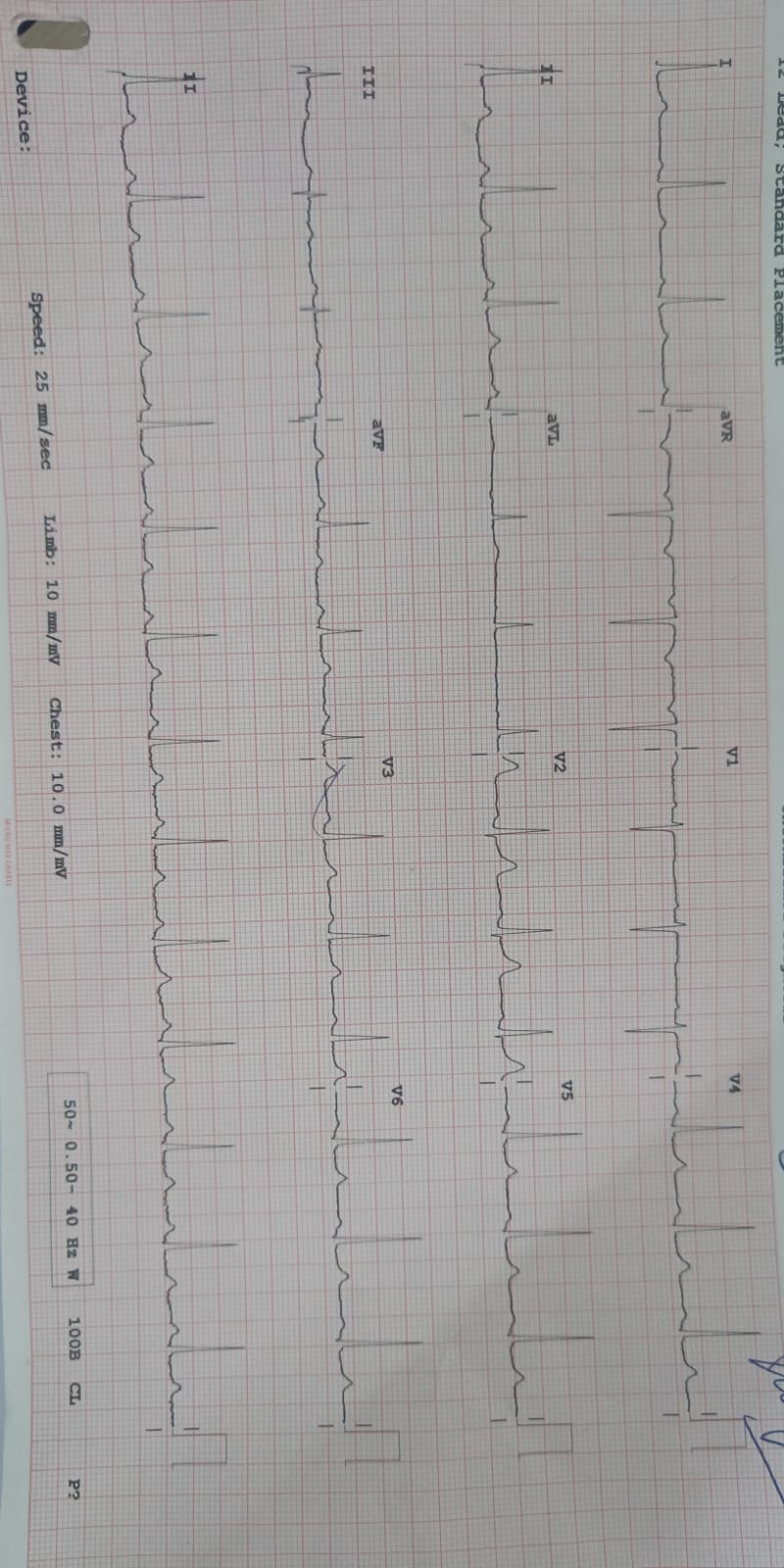
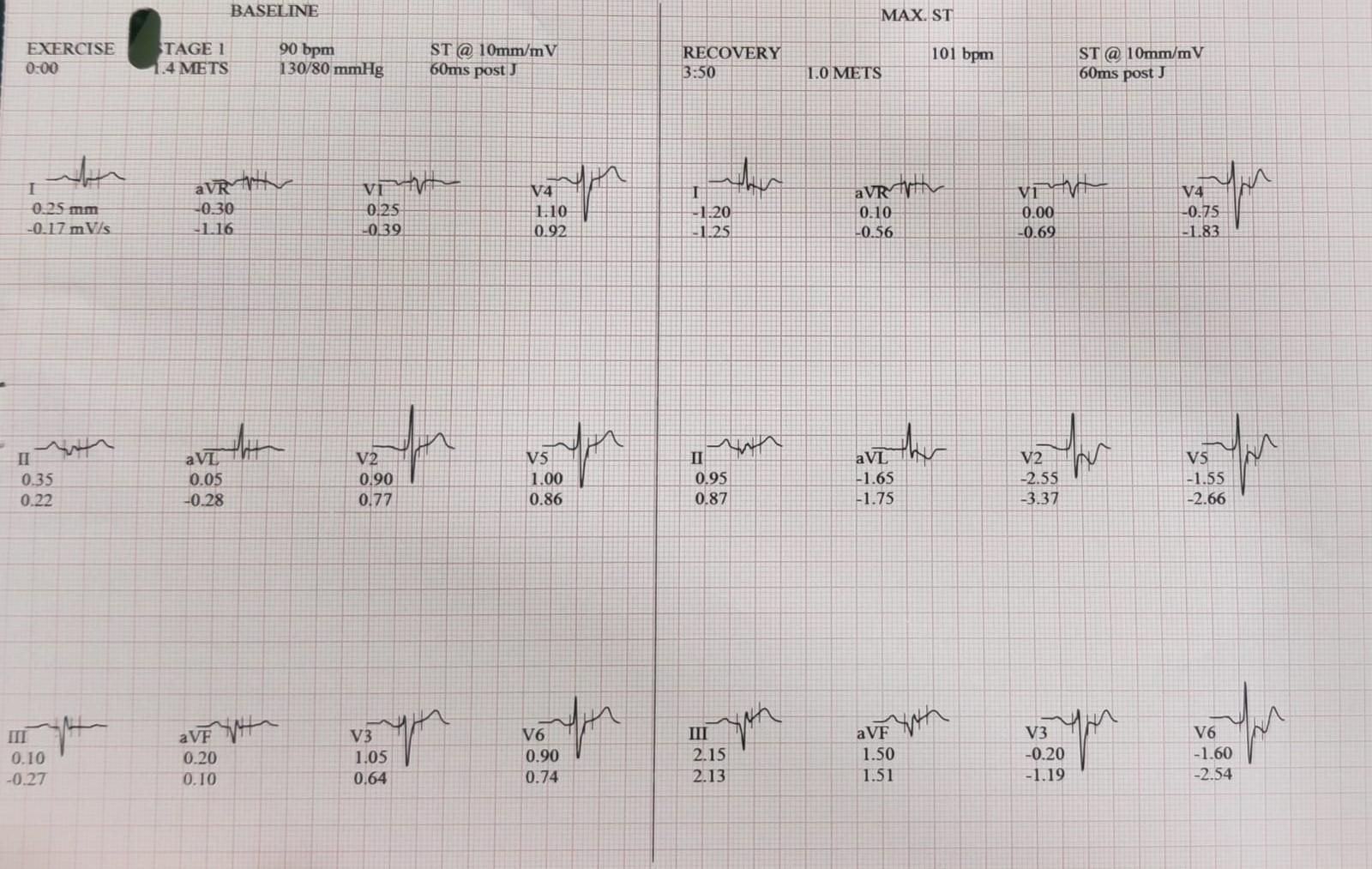
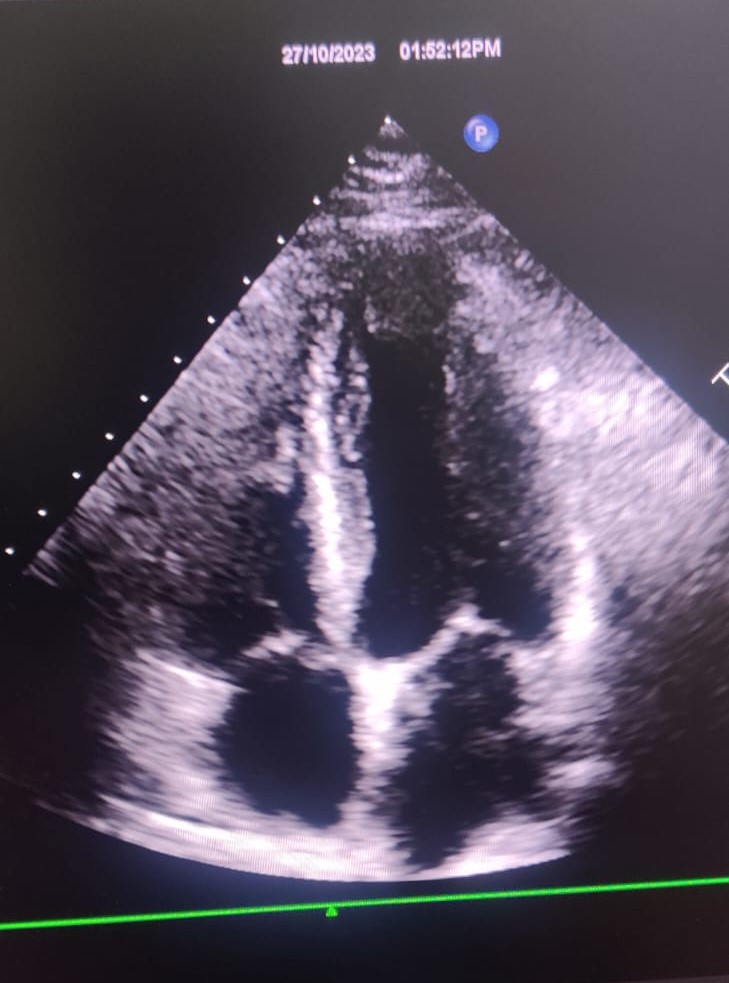
68 year old male with recent onset angina, New York Heart Association Class III. Heart rate 64 beats per minute. Blood Pressure 120/70 mm Hg. Electrocardiogram – Normal. Treadmill test – Positive. LVEF – 60%.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
Left Main Coronary Artery - Normal. LAD – Type III with 50 – 60% lesion in mid segment across D1. LCX – Large, non dominant with 50% lesion before OM 1 followed by 50% long lesion in distal LCX having small caliber. RCA – Dominant, severely calcified with 90% lesion in proximal segment followed by 95% long lesion after RV branch. Impression: Critical single vessel coronary artery disease. Plan: PCI to RCA with Rotablation.

Interventional Management
Procedural Step
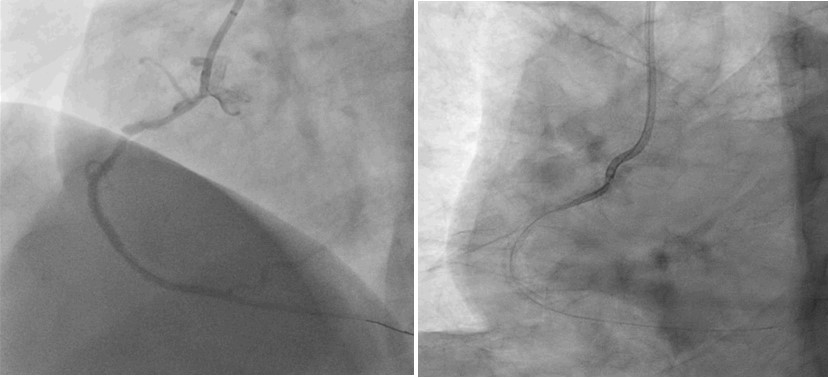
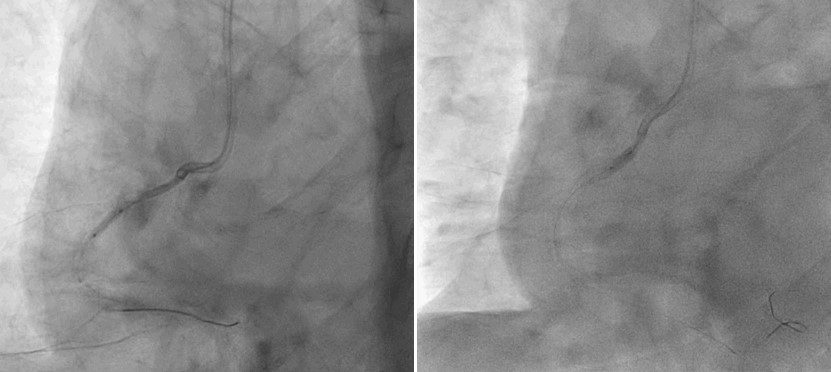
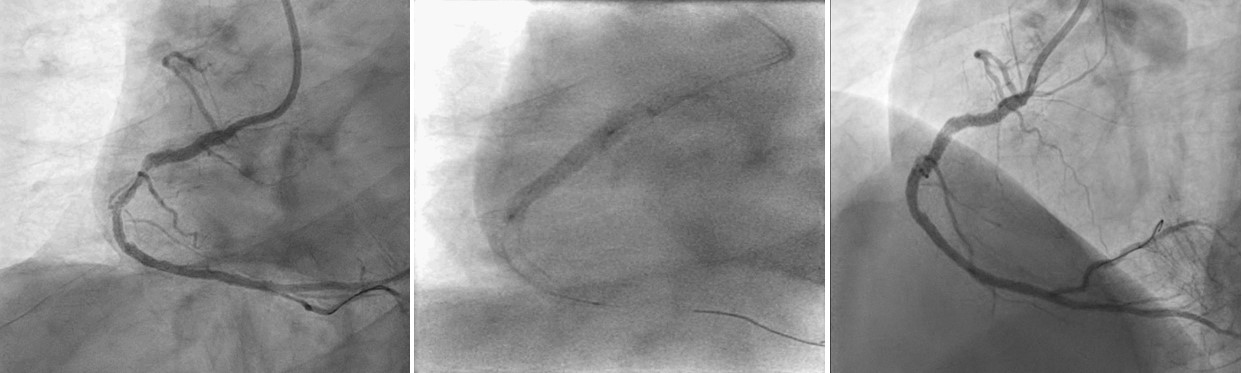
6 F JR 3.5 guiding was used. BMW wire was advanced into distal RCA. Proximal lesion was predilated with 2 x 15 mm Ryurei at 12 atm. Rotablation was deferred in view of smooth passage of balloon and dissection from previous dilatation. Distal lesion couldn’t be negotiated, so Grand Slam J was advanced in distal RCA and then lesion was predilated with 2 x 10 mm Ryurei. Proximal RCA redilated with 2.5 x 12 mm Accuforce (Terumo, Japan) over BMW wire at 14 atm with Guidezilla II (Boston, USA) support. While attempting parallel wire technique with Grand Slam J, the whole system got disengaged. The guiding was changed to 6 F Amplatz 1 (Cordis, USA) and RCA was rewired with BMW wire. Serial predilatations were done. 2.75 x 24 mm Ultimaster Tansei was deployed with Guidezilla support in mid RCA. 2.75 x 28 mm Ultimaster Tansei was advanced into proximal RCA but it got dislodged into ostium because of calcium and poor support. BMW wire was exchanged with OTW system along with 1.20 x 08 mm Mini Trek OTW (Abbott, USA) in order to have extra support, proper advancement through uninflated stent with simultaneous administration of contrast. 1.20 x 08 mm balloon was inflated inside the dislodged stent. With series of gradual inflations of varying balloon sizes, the stent was deployed in proximal RCA. With Guidezilla support, 3.0 x 18 mm Ultimaster Tansei was deployed in between the two stents, overlapping both the stents and post dilated with 3.0 x 08 mm Accuforce to achieve TIMI III flow.
Case Summary
Stent dislodgement is rare (0.9 to 8.3 %) but potentially serious complication of PCI. Factors include tortuosity and calcification. Conventional bail out methods include passage of small balloon, double wire technique, snaring or crush technique. Rotablation was deferred in view of smooth passage of balloon. Stent was trapped in calcium and dislodged due to non coaxial guide support. Guidezilla and OTW system helped for additional support for the wire, to administer contrast to confirm instent wire positioning and for wire exchange. Usually, dislodged stent is retrieved or crushed. We deployed same stent successfully with small balloon technique which is rare.