
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-223
Symptomatic Severe Mitral Stenosis in a Pregnant Lady
By Su Min Lim
Presenter
Su Min Lim
Authors
Su Min Lim1
Affiliation
Hospital Pulau Pinang, Malaysia1,
View Study Report
TCTAP C-223
Structural - Other Structural Interventions
Symptomatic Severe Mitral Stenosis in a Pregnant Lady
Su Min Lim1
Hospital Pulau Pinang, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
25 yr old lady C/O SOB , treated by district hospital as AEBA CXR from district hospital show cardiomegaly and given frusemide and improved

Relevant Test Results Prior to Catheterization
TOE done showed Severe MR with MVA planimetry 0.66 and MPG 30
Relevant Catheterization Findings
Interventional Management
Procedural Step
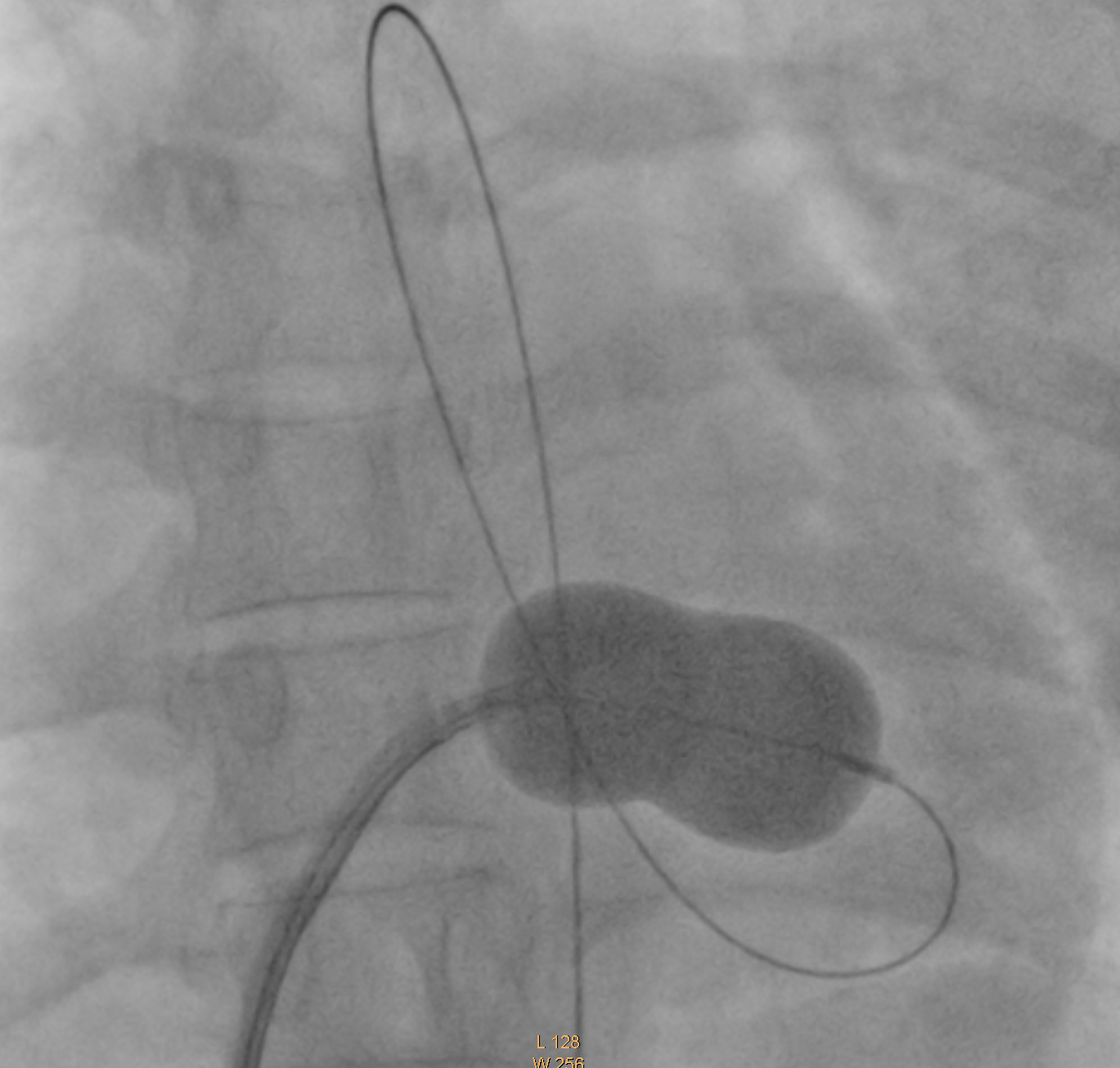
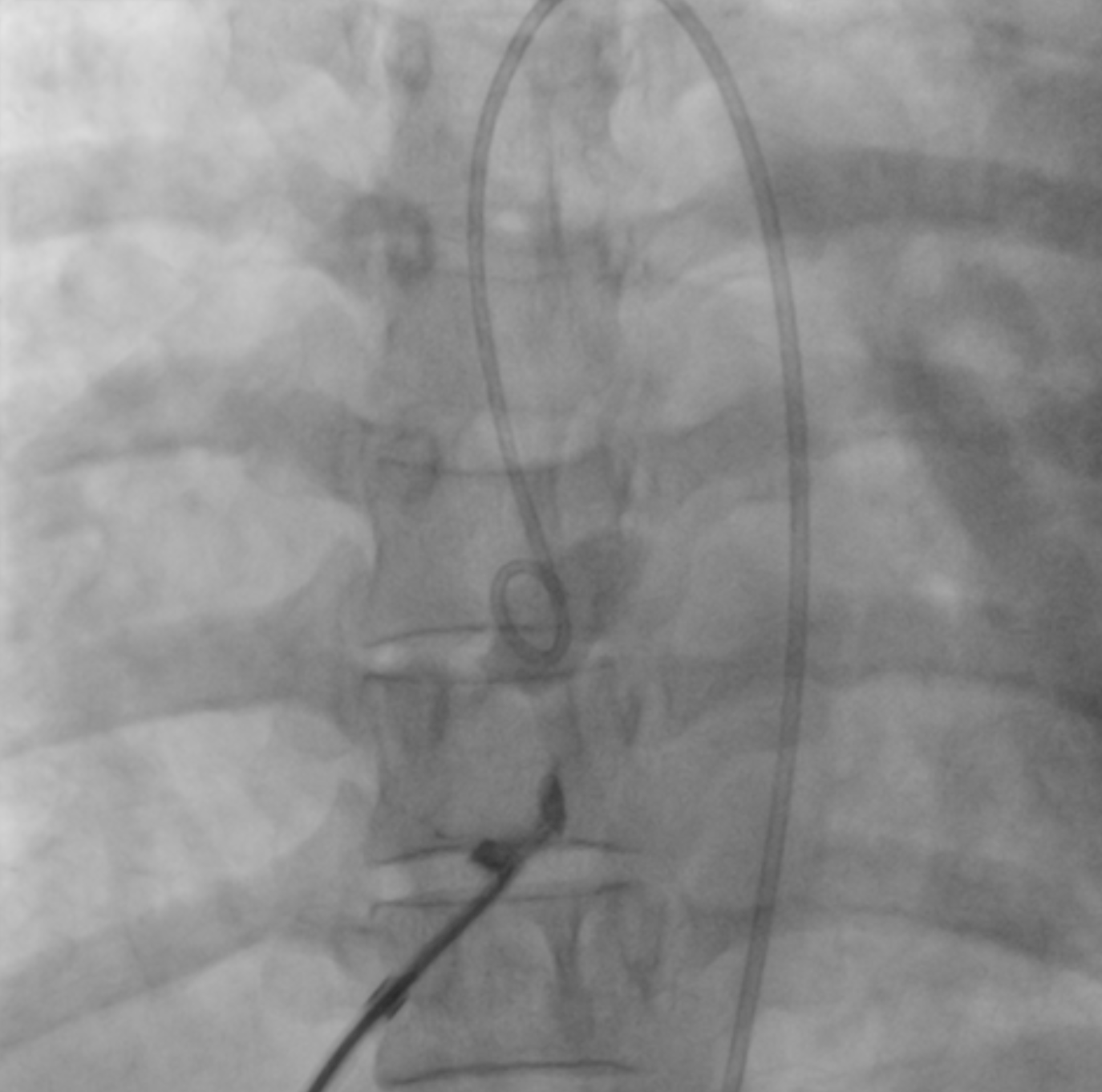
Abdominal shield and peri operative TTE 6Fr pigtail at Ao, RA gram and follow Transseptal puncture under fluoroscopy guidance Wollie wire to LA PTMC inouoe balloon intrpduced but unable to direct to MVdespite manipulation – likely due to low septal puncture Decided to create AV loop- long terumo wire RA-LA-LV-AO Successfully crossed MV Balloon inflation X2 (26 mm) Well tolerated with transient hypotension Rpt ECHO MVA 1.53cm2 MPG 8mmHg, no pericardial effusion
Case Summary
Low septal puncture in this case resulting difficulties to direct the balloon to MV- should aim high posterior puncture
Snare and create AV looping to facilitate the movement into MV is an potential solution in this case than redo transseptal puncture
Snare and create AV looping to facilitate the movement into MV is an potential solution in this case than redo transseptal puncture