
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-220
The Challenging Cardiac Structural Interventional Mission: A Percutaneous Transluminal Mitral Commissurotomy in a Patient With an IVC Filter
By Thanaphruet Issarawattana, Tawai Ngernsritrakul, Krissada Meemook
Presenter
Thanaphruet Issarawattana
Authors
Thanaphruet Issarawattana1, Tawai Ngernsritrakul1, Krissada Meemook2
Affiliation
Ramathibodi Hospital, Thailand1, Ramathibodi Hospital Mahidol University, Thailand2,
View Study Report
TCTAP C-220
Structural - Other Structural Interventions
The Challenging Cardiac Structural Interventional Mission: A Percutaneous Transluminal Mitral Commissurotomy in a Patient With an IVC Filter
Thanaphruet Issarawattana1, Tawai Ngernsritrakul1, Krissada Meemook2
Ramathibodi Hospital, Thailand1, Ramathibodi Hospital Mahidol University, Thailand2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 66-year-old woman presented with dyspnea on exertion for 2 months. She had complete remission of cervical cancer following a course of chemotherapy, radiation, and surgery. She had a medical history of deep venous thrombosis on an IVC filter and warfarin. Physical examination showed a diastolic rumbling murmur grade II with an opening snap at the apex. Chest X-ray showed cardiomegaly with a widening carina angle without congestion. ECG showed sinus rhythm without remarkable abnormalities.

Relevant Test Results Prior to Catheterization
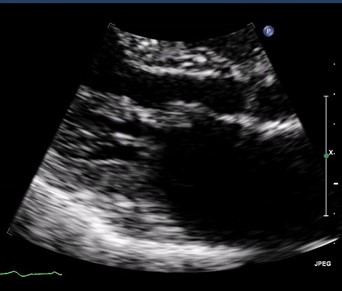
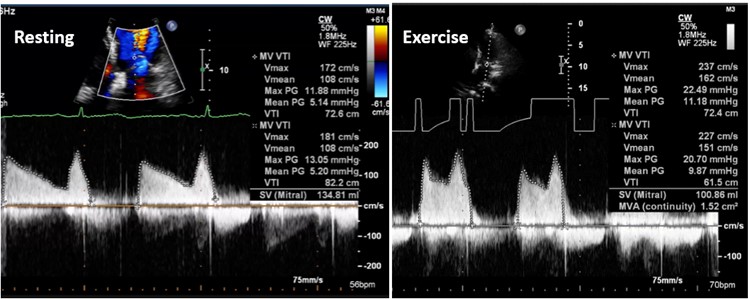
The echocardiography revealed normal ventricular systolic function with moderate left atrium dilation, and a fish mouth appearance with diastolic doming of the mitral valve. A mean pressure gradient of 6 mmHg across MV, with mitral valve area of 1.5 cm2 and a Wilkin score of 6. Following a bicycle stress test, the mean pressure gradient increased to 11 mmHg. The patient was diagnosed with symptomatic severe rheumatic MS. A percutaneous transluminal mitral commissurotomy was scheduled.
Relevant Catheterization Findings
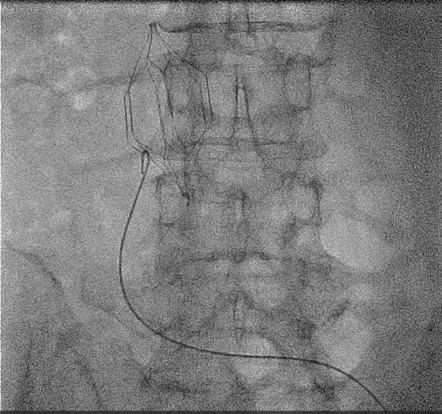
A 6 F sheath was inserted via the left femoral vein. A 0.035-inch J-tip wire was advanced to the right atrium. However, the transseptal guiding introducer sheath could not pass through the IVC filter. An IVC venography revealed complete endothelialization of the IVC filter with an intraluminal filling defect at the lower part, consistent with the IVC thrombus. Consequently, the procedure was halted, and an alternative approach was adopted, using venous access through the internal jugular vein.


Interventional Management
Procedural Step
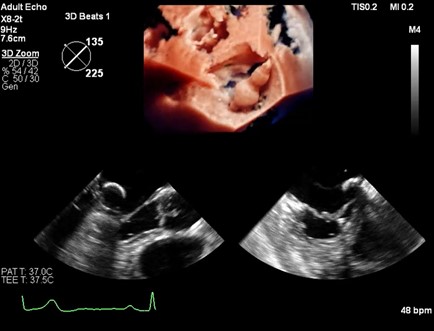
Under light sedation and local anesthesia, transesophageal echocardiography revealed no left atrium thrombus. A 5 F sheath was inserted via the right femoral artery to place the pigtail catheter in the left ventricle for measurement. Following this, an 8.5 F transseptal guiding introducer sheath (SL-0TM, St Jude Medical) was inserted via the right internal jugular vein for trans-septal puncture of the interatrial septum using a Brockenbrough needle, guided by echocardiography. The SL-0 sheath was then advanced to the left atrium, and a 0.025-inch stainless steel coiled-tip wire was inserted. After removing the SL-0 sheath, a trans-septal 12F dilator was advanced to widen the right neck entry route and the interatrial septum. Subsequently, the Inoue balloon catheter was introduced over the coiled tip wire into the left atrium and a stylet was used to manipulate it. Upon the balloon crossing the mitral valve; the distal portion was inflated, and the balloon was retracted to anchor in the mitral valve, followed by inflation to a maximum diameter of 26 mm. During echocardiography, the gradient across MV decreased from 8 to 3 mmHg with mild mitral regurgitation and no evidence of pericardial effusion. The patient was discharged the next day with a significant improvement in symptoms. Subsequent follow-up echocardiography revealed residual mild mitral stenosis after a span of three years.


Case Summary
The transjugular venous approach for percutaneous transluminal mitral commissurotomy is a safe, feasible, and effective alternative in treating symptomatic rheumatic mitral stenosis, potentially avoiding the need for surgery.