
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-023
Bidirectional Orbital Atherectomy for Treatment of Diffuse and Calcified Coronary Artery Disease
By Gavin Ng, Hui Wen Sim, Jieli Kua
Presenter
Gavin Ng
Authors
Gavin Ng1, Hui Wen Sim1, Jieli Kua2
Affiliation
National University Heart Centre, Singapore1, Ng Teng Fong General Hospital, Singapore2,
View Study Report
TCTAP C-023
Coronary - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Bidirectional Orbital Atherectomy for Treatment of Diffuse and Calcified Coronary Artery Disease
Gavin Ng1, Hui Wen Sim1, Jieli Kua2
National University Heart Centre, Singapore1, Ng Teng Fong General Hospital, Singapore2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Madam AR is a 79 year old female who presented in March 2022 with Non-ST-elevation myocardial infarction complicated by acute pulmonary oedema. She has diabetes, hypertension and chronic kidney disease. She also has peripheral vascular disease, and old cerebrovascular disease. Angiogram showed diffuse and calcified left anterior descending (LAD) artery disease and she was deemed too high risk for surgery. She was scheduled for percutaneous coronary intervention (PCI).

Relevant Test Results Prior to Catheterization
Echocardiogram done during the admission showed a left ventricular ejection fraction of 50% with moderate mitral regurgitation. Her haemoglobin and creatinine levels were at her baseline of 11 g/dl and 140 mmol/L respectively.
Relevant Catheterization Findings
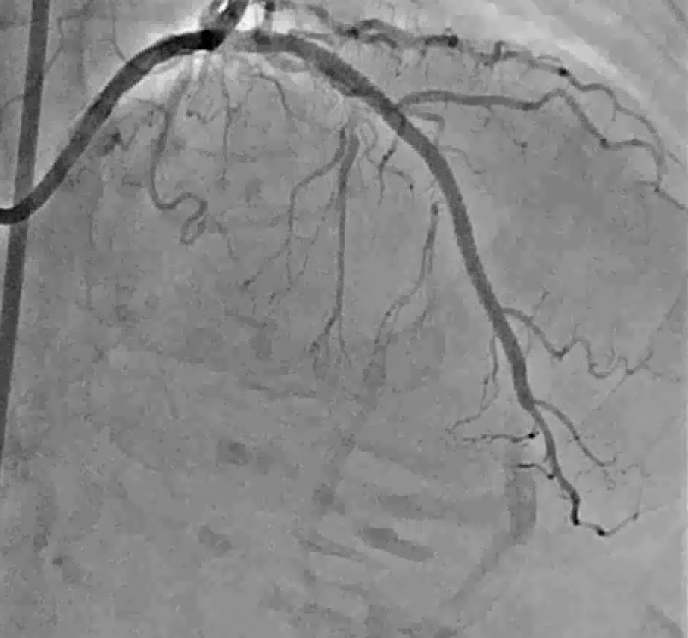
Initial diagnostic angiogram revealed a severely calcified and diffuse LAD artery disease. There were also severe stenoses in the right posterior descending and distal left circumflex arteries. A multidisciplinary meeting involving cardiothoracic surgeons and interventional cardiologists reviewed the case and the proposed action was for PCI to the LAD and symptom guided therapy for the residual disease.
Interventional Management
Procedural Step
Femoral access was chosen in view of radial artery spasm. The left coronary ostium was cannulated with a 7 Fr EBU 3.5 guide catheter. A Runthrough NS guidewire loaded onto a Corsair Pro XS microcatheter was used to wire into the distal LAD. Intravascular ultrasound (IVUS) using the 60 MHz Opticross HD catheter was attempted but this could not cross the mid LAD lesion, indicating the point of tightest stenosis. The Runthrough wire was exchanged out for the ViperWire. Thereafter, orbital atherectomy using the Diamondback 360 Coronary Orbital Atherectomy System was performed antegradely from the mid LAD to distal LAD followed by retrogradely from the mid to proximal LAD. This was done stepwise to minimize the risk of no-reflow due to the diffusely calcified disease. The lesion was further prepared using appropriately sized non-compliant and scoring balloons. Thereafter, 2 drug eluting stents were implanted sequentially from the proximal to distal LAD and the result was optimized with IVUS. The minimal lumen area in the proximal LAD was 1.9 mm2 and the corresponding minimal stent area improved to 7.0 mm2 after PCI. 50 mls of contrast was used judiciously during the procedure and this minimized the risk of contrast induced nephropathy.

Case Summary
This case illustrates the effective treatment of a diffuse and calcified LAD artery using bidirectional orbital atherectomy. This technique reduces the risk of slow and no-reflow by preparing the lesion distally before more debulking is done proximally. IVUS can guide the precise deployment of stents and optimize the PCI result by ensuring that the stents are well apposed and expanded. At 1 year review, the patient remains well with no reported symptoms and the renal function remained stable.