
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-067
Complex CTO With Epicardial Collaterale Retrograde Which Is the Best Approach?
By Mahesh Shivaji Ahire
Presenter
Mahesh Shivaji Ahire
Authors
Mahesh Shivaji Ahire1
Affiliation
SMBT Heart Institute, Nashik, Maharashtra, India, India1,
View Study Report
TCTAP C-067
Coronary - Complex PCI - CTO
Complex CTO With Epicardial Collaterale Retrograde Which Is the Best Approach?
Mahesh Shivaji Ahire1
SMBT Heart Institute, Nashik, Maharashtra, India, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
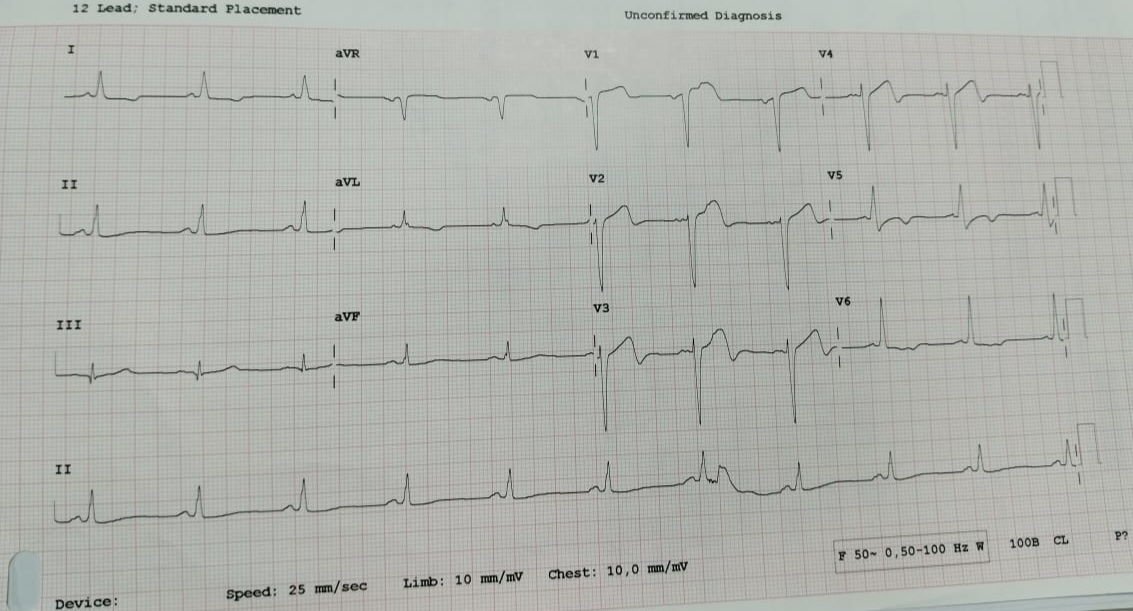
44 yrs/ Male Anterior wall Myocardial Infarction [2021]Attempted PTCA to LAD on 17/6/2021Echo s/o Ischemic Heart Disease LVEF 30% Lad territory akinetic with preserved wall thicknessMild MR , NO PAHOn regular medication
Relevant Test Results Prior to Catheterization
2D ECHO s/o Ischemic Heart Disease LVEF 30% Lad territory akinetic with preserved wall thicknessMild MR, No PAH



Relevant Catheterization Findings
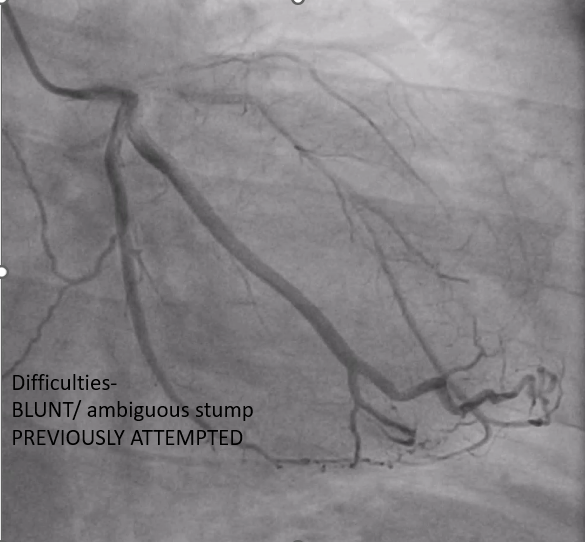
CORONARY ANGIOGRAPHY SINGLE VESSEL DISEASE LAD VESSEL CTO LESION RETROGRADLY FILLING WITH MAJOR VESSEL OM AMBIGUOUS CTO CAP , BLUNT TIP LCX DOMINANT VESSEL NORMAL RCA NON DOMINANT NORMAL
Interventional Management
Procedural Step
DIFFICULTIES-BLUNT/AMBIGUOUS STUMP PREVIOUSLY ATTEMPTED.
44 MM DES WAS TAKEN OVERLAPPING WITH EARLIER STENT 2.5X44MM SIROLIMUS DRUG ELUTING STENT

44 MM DES WAS TAKEN OVERLAPPING WITH EARLIER STENT 2.5X44MM SIROLIMUS DRUG ELUTING STENT
Case Summary
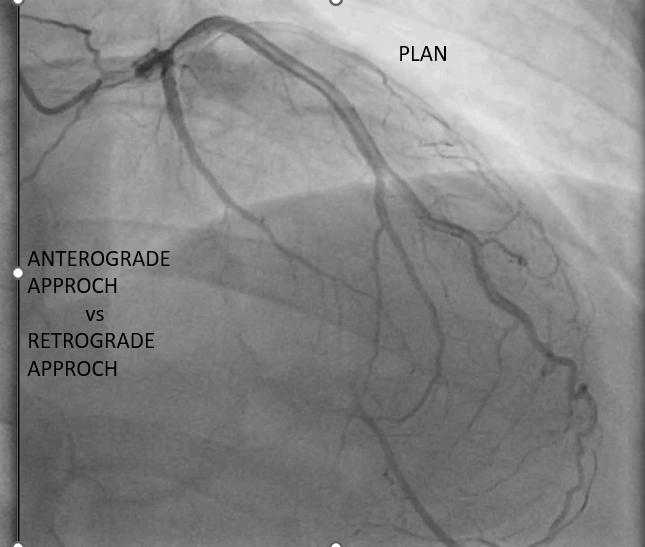
1. RETROGRADE APPROACH IS A GOOD OPTION FOR CTO, provided we handle them very carefully2. antegrade should be the preferred approach.3.Wire escalation should be done carefully depending on lesion subsetHardware including snares/wires/microcatheters/guide catheter are key for complex interventions