
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-161
Negotiating the Tortuosities : PCI in a Female With Arteria Lusoria
By Wickramasinghe Wasala Mudiyanselage Pasan Aminda B Abeysenevi, Mohamed Basheer Fasllur Rahuman, Nimali Fernando, Leonard Wanninayake, Chathurika Samarakoon Kempitiya B.C.T.A.N.W.M.R
Presenter
Wickramasinghe Wasala Mudiyanselage Pasan Aminda B Abeysenevi
Authors
Wickramasinghe Wasala Mudiyanselage Pasan Aminda B Abeysenevi1, Mohamed Basheer Fasllur Rahuman1, Nimali Fernando2, Leonard Wanninayake1, Chathurika Samarakoon Kempitiya B.C.T.A.N.W.M.R3
Affiliation
National Hospital of Sri Lanka, Sri Lanka1, Nawaloka Hospital Colombo, Sri Lanka2, Dr, Sri Lanka3,
View Study Report
TCTAP C-161
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
Negotiating the Tortuosities : PCI in a Female With Arteria Lusoria
Wickramasinghe Wasala Mudiyanselage Pasan Aminda B Abeysenevi1, Mohamed Basheer Fasllur Rahuman1, Nimali Fernando2, Leonard Wanninayake1, Chathurika Samarakoon Kempitiya B.C.T.A.N.W.M.R3
National Hospital of Sri Lanka, Sri Lanka1, Nawaloka Hospital Colombo, Sri Lanka2, Dr, Sri Lanka3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Ms.SA, a 59 year-old female with T2DM, hypertension and CKD presented to the ETU with worsening angina at rest over 4 hours with autonomic symptoms. She had a history of ischemic heart disease and PCI being done in 2016. Past records were unavailable. She had diabetic micro & macro-vascular complications due to poor follow-up.She was haemodynamically stable despite severe pain. Peripheral pulses were poor except for right ulnar pulse. She was obese & had intertrigo at inguinal regions.

Relevant Test Results Prior to Catheterization
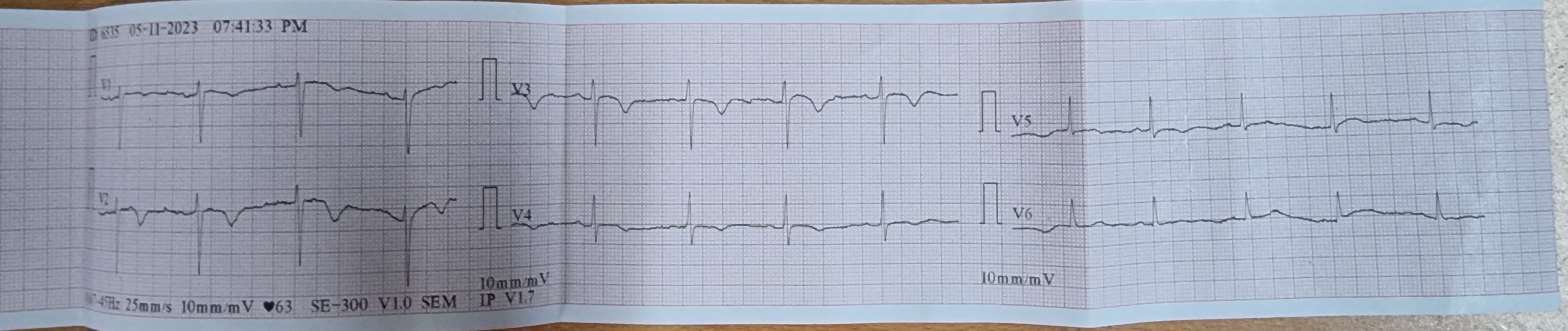
The ECG revealed deep T inversions in V2 and V3 leads suggestive of a Wellens type B pattern which was not seen in her previous ECGs. The troponin I level was markedly elevated (>100 ULN). A Bed side 2D echocardiogram was done. This showed an ejection fraction of 45% with anterior and apical hypokinesia with preserved muscle mass. She had mild anaemia with a haemoglobin level of 10g/dl. Other cell lines were normal. Serum creatinine was 1.5umol/l.Liver transaminases were marginally elevated.

Relevant Catheterization Findings
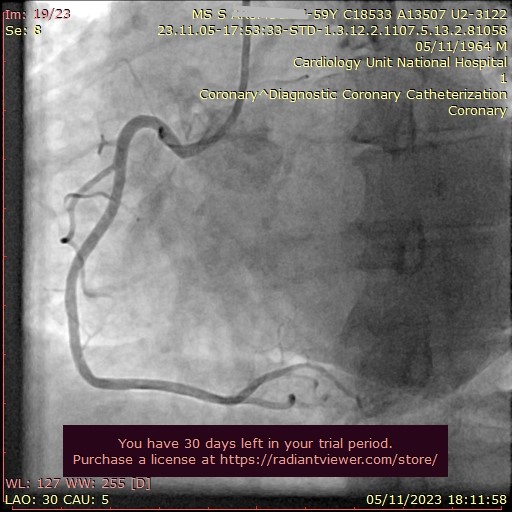
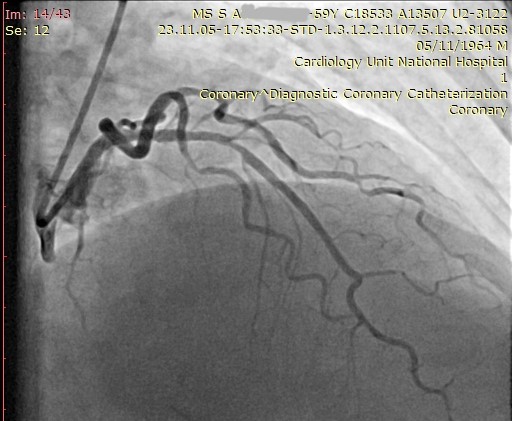
6FG Right ulnar arterial sheath was inserted. The long guide wire kept entering the descending aorta even with special manoeuvres . Dye was injected to delineate the vascular anatomy which revealed Arteria Lusoria. The stiff guide wire was exchanged to a hydrophilic TERUMO long guide wire. LMCA could not be engaged with the TIGER catheter. RCA was normal. 6F EBU GC could not be advanced. A 5F BL catheter was used to engage the LMCA. LAD had severe plaque disease just distal to the stent.


Interventional Management
Procedural Step
As this was an acute presentation with a high risk NSTEMI, it was decided to stent the proximal LAD lesion. Since the prior attempts to advance the 6FG EBU 3 guide catheter to the aortic root ended up in failure with the stiff long guide wire prolapsing in to the descending aorta, we had to resort to the 5FG BL guide catheter to carry out the PCI. Torquing of the catheter with deep breath holding helped us obtain a deep engagement with sufficient catheter support.LAD was wired with an ASAHI SION Blue 0.014" guide wire. The lesion just adjacent to the previous stent was pre-dilated with a SAPPHIRE 2 X 12mm compliant balloon up-to 10 atm. A RESOLUTE INTEGRITY 4 X 18mm drug eluding stent was deployed at nominal pressure overlapping the distal end of the previous LAD stent. Stent was post-dilated with a non compliant balloon for optimal results. All this could be done via the 5FG guide catheter thanx to the sufficient support obtained from the BL guide catheter. Post-procedure angiogram revealed good results with TIMI III flow in LAD and it's branches. Patient was kept on dual antiplatelets and a high intensity statin.


Case Summary
Although PCI via radial access let alone ulnar access is considered a relative contra-indication in patients with Arteria Lusoria, the presence of peripheral vascular disease and severe inguinal intertrigo necessitated such an intervention. This is a perfect example of situational adaptation along with utilization of procedural skills & available resources. It is of utmost importance that proper documentation of procedures are made including difficulties faced & the techniques used to overcome those. Steps should always be taken to minimize risk to the patient while ensuring maximum benefit.