
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-048
Successful Staged PTCA of Complex CTO of LAD and RCA in A Patient With Multivessel Coronary Artery Disease and Severe LV Dysfunction
By Saurabh Goel, Dr Ashish Goel
Presenter
Saurabh Goel
Authors
Saurabh Goel1, Dr Ashish Goel2
Affiliation
Wockhardt Hopsital, Mumbai Central, India1, Symbiosis Hospital Dadar, Mumbai, India2,
View Study Report
TCTAP C-048
Coronary - Complex PCI - CTO
Successful Staged PTCA of Complex CTO of LAD and RCA in A Patient With Multivessel Coronary Artery Disease and Severe LV Dysfunction
Saurabh Goel1, Dr Ashish Goel2
Wockhardt Hopsital, Mumbai Central, India1, Symbiosis Hospital Dadar, Mumbai, India2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 50 year old male , MR M M, admitted with history of progressive breathlessness since one month, increasing over the last 3 days with orthopnea and edema feet. He is non diabetic with past history of HT. He was admitted to ICCU as a case of Ischemic LVF. Clinical examination revealed HR 110/min, BP 110/70 CVS – Tachycardia noted, RS – Bilateral crepts noted. Oxygen Saturation was 92%on room air.
Relevant Test Results Prior to Catheterization
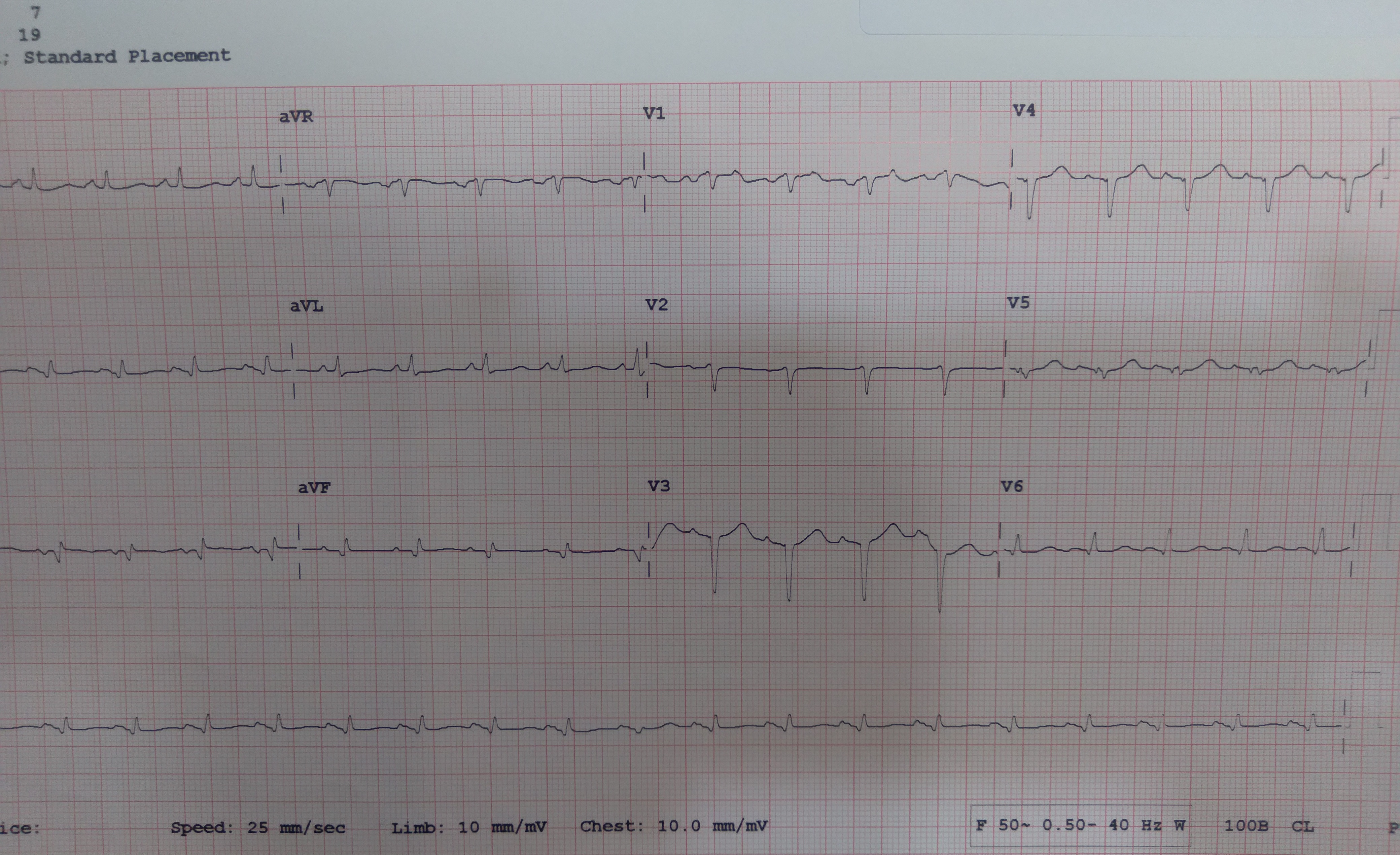
ECG – showed evolved anterior myocardial infarction. NT-Pro BNP was markedly elevated= 5120 pg/mL, CPK MB and Troponin I was normal and creatinine was elevated = 1.8 Mg/DL. 2 D echo – LV showed dilatation with preserved thickness of myocardial segments, LV ejection fraction was 20 %,distal septal , apical and inferolateral marked hypokinesia, Marked diastolic dysfunction was noted .He was stabilized with medical treatment for two days and then taken for coronary angiography.


Relevant Catheterization Findings
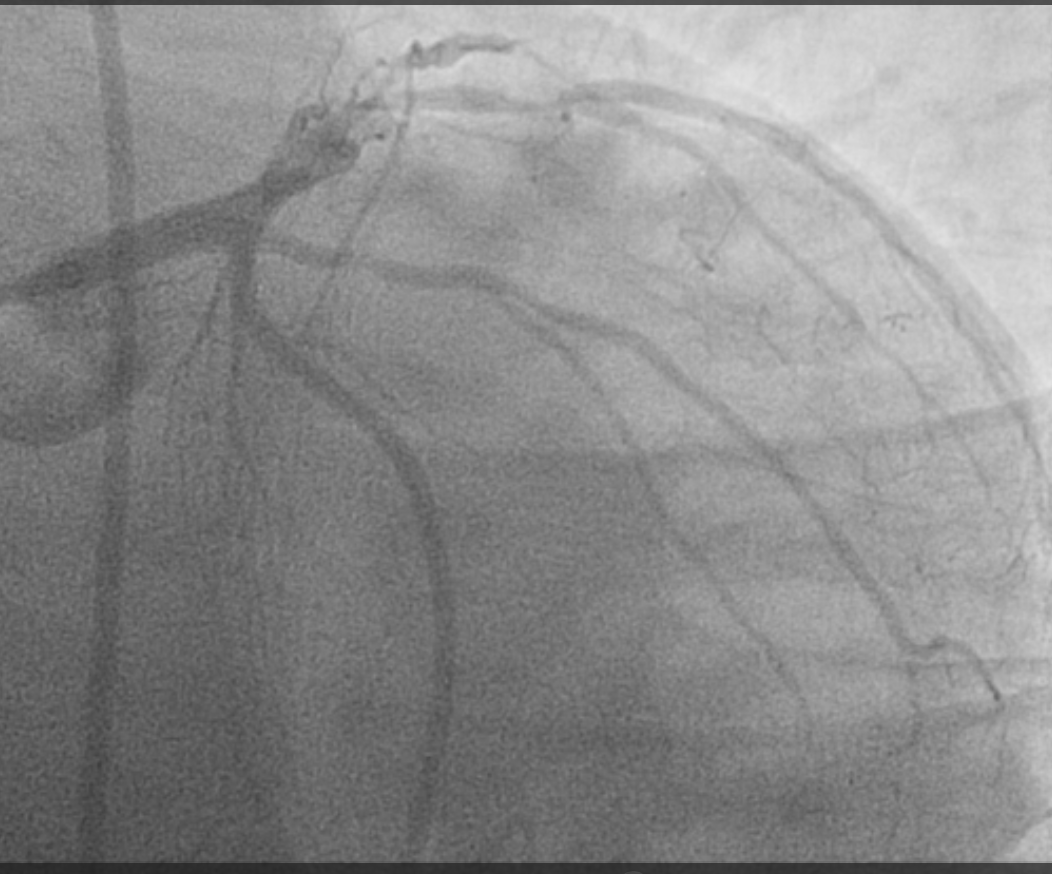
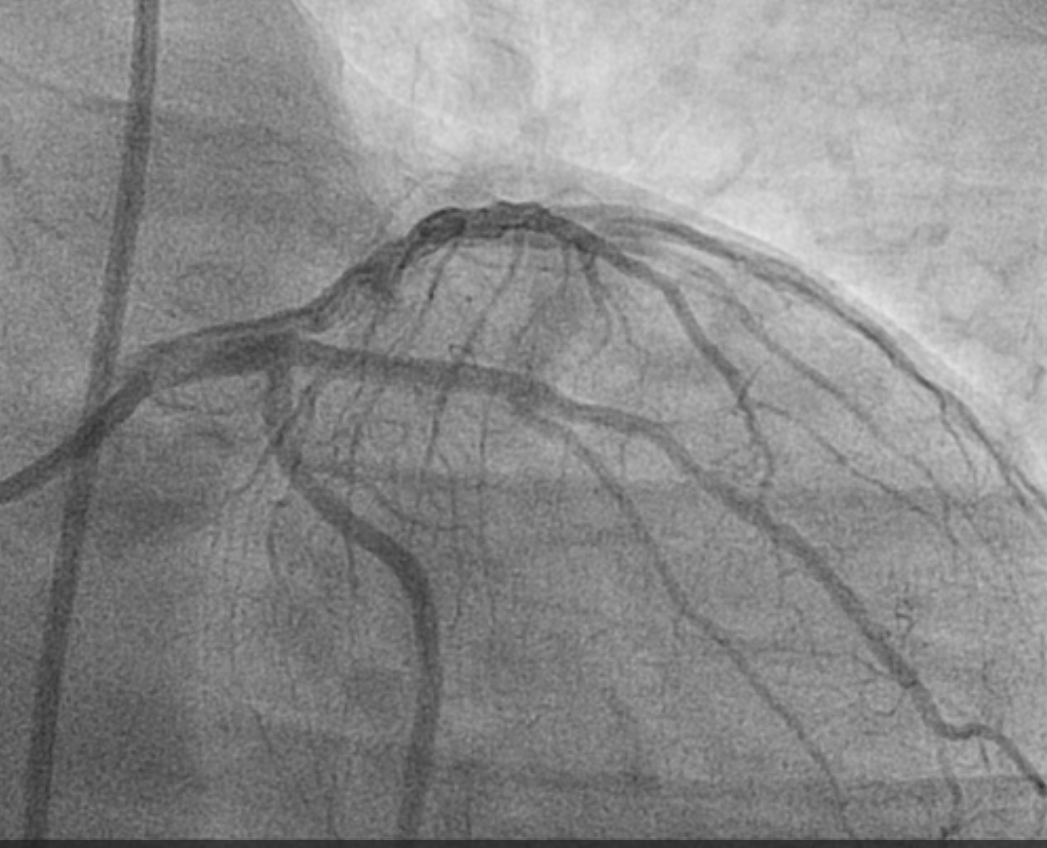
Angiography was done from right femoral route Left Main– normal. LAD - Showed Mid total occlusion Proximal septal branches of LAD give collaterals to distal RCA. LCx - is non dominant with plaques. Ramus –Showed proximal discrete 90% lesion. RCA – dominant large vessel with proximal ectasia and multiple proximal and mid segment near total occlusions.


Interventional Management
Procedural Step
First stage PTCA of LAD was taken up. The left coronary artery was cannulated using 6F EBU 3.5 guiding catheter . The crossing of LAD lesion was attempted with Turn trak wire , however the lesion could not be crossed. Then Gaia I wire was used which crossed the lesion. Predilatation was done with 2.0X 15 mm followed by 2.5mm X 15 mm balloon and then the Gaia wire exchanged for Turn Trak wire. Stenting of the LAD was done 2.75X 28 mm Xience stent and it was post dilated with 3 X 12 balloon. Good TIMI 3 flow was achieved in LAD. The patient on follow up after few weeks showed good clinical improvement and LV ejection fraction to improved 30%. Staged PCI of Ramus and RCA were done after few weeks. The Ramus lesion was predilated with 2.0 X 12 mm balloon followed by stenting with 2.5X 23 Xience stent . The crossing of RCA lesion was attempted with Pilot wire, followed by Fielder XT wire , however the lesion could not be crossed. Finally Gaia II wire was used with microcatheter support and the lesions were successfully crossed. Predilatations were done serially with 2.0X12 and 2.75X 15 balloons and good antegrade flow established in RCA. The Gaia wire was exchanged for Turn Trak wire. Stenting was done 2.75 X 28 Xience stent in mid RCA, followed by 3.5 X 38 in proximal RCA overlapping the distal stent. Final post dilatation was done with 3.5X15 mm balloon with good result.


Case Summary
This case demonstrates that in the situation of severe ischemic cardiomyopathy , complex multivessel disease was tackled in staged procedures. The right coronary anatomy was very challenging due to proximal ectasia, multiple bends and three successive CTO lesions from proximal to Mid RCA. Antegrade approach entailed the use of use of various wires with microcatheter support and final crossing was achieved with Gaia wires in LAD and RCA. Good revascularization was achieved with improvement in clinical status and LV function of the patient. Two CTO lesions were effectively tackled with appropriate hardware.