
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-017
Simultaneous Double Vessels Acute Total Occlusion
By Ng Kwang How, Ahmad Syadi Mahmood Zuhdi, Alexander Loch
Presenter
Ng Kwang How
Authors
Ng Kwang How1, Ahmad Syadi Mahmood Zuhdi2, Alexander Loch2
Affiliation
University Malaya Medical Center, Malaysia1, University Malaya Medical Centre, Malaysia2,
View Study Report
TCTAP C-017
Coronary - ACS/AMI
Simultaneous Double Vessels Acute Total Occlusion
Ng Kwang How1, Ahmad Syadi Mahmood Zuhdi2, Alexander Loch2
University Malaya Medical Center, Malaysia1, University Malaya Medical Centre, Malaysia2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Mr M, a 47-year-old foreign male smoker, without known medical illnesses, was referred from a private hospital for acute inferior myocardial infarction due to financial constraint. He presented with acute onset of typical chest pain at 4am, associated with diaphoresis and shortness of breath. His vital signs were stable, BP 148/72mmHg, Heart rate 84beats/min, SpO2 95%. Cardiovascular and respiratory examinations were unremarkable.
Relevant Test Results Prior to Catheterization
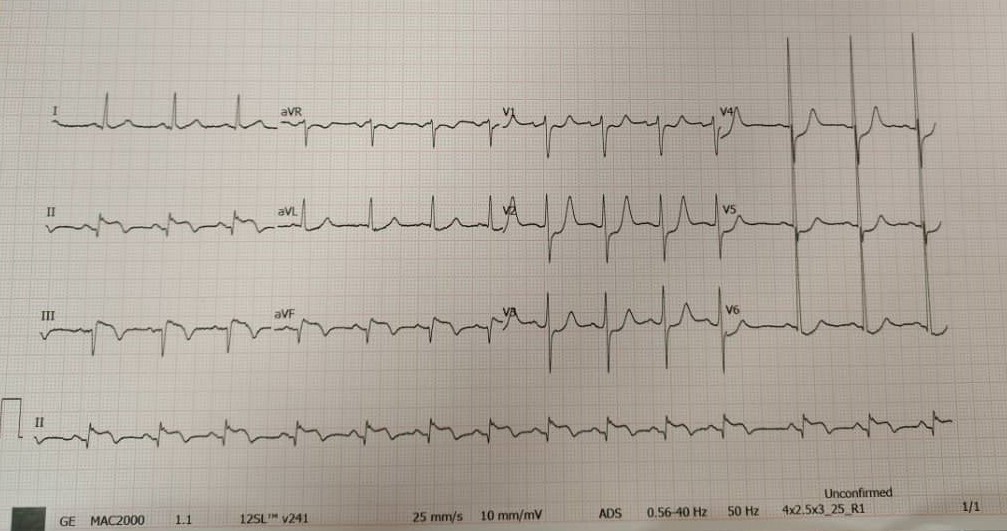
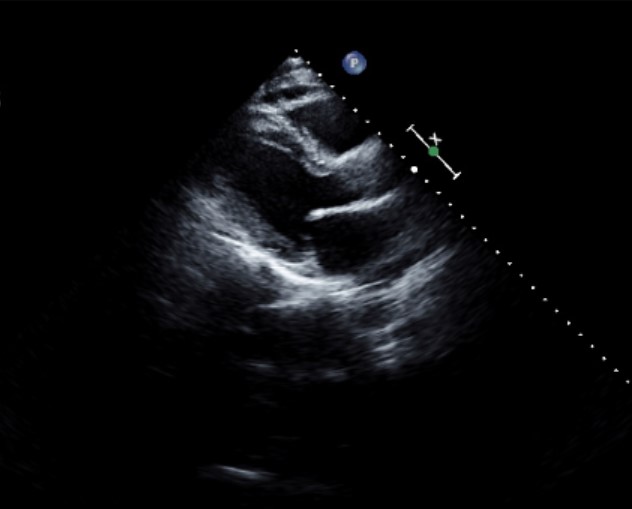
His ECG showed ST elevation over leads II,III and AVF. Echocardiography showed LVEF 40-45%, regional wall motion abnormality over inferolateral region, normal chamber size, no pericardial effusion or intracardiac thrombus.Trop I 5005 ng/L, Creatinine 68 umol, Hemoglobin 16.8 g/L, LDL 2.89 mmol/L.
Relevant Catheterization Findings
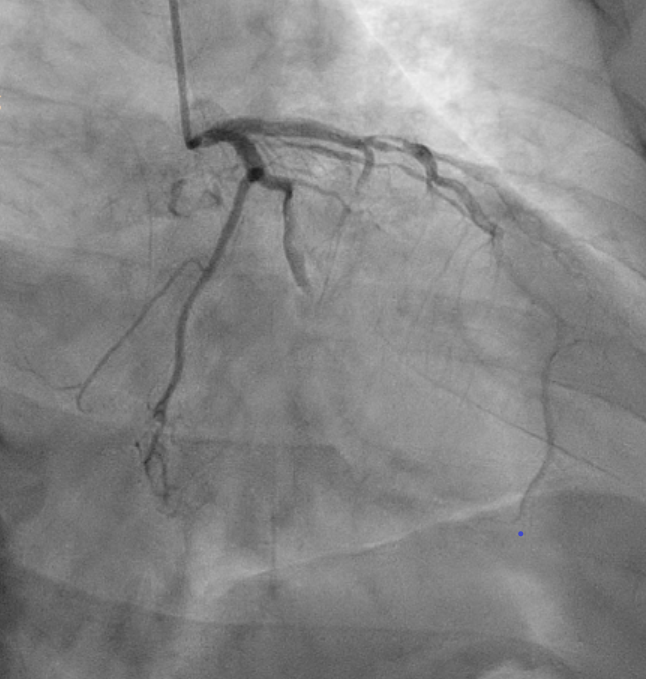
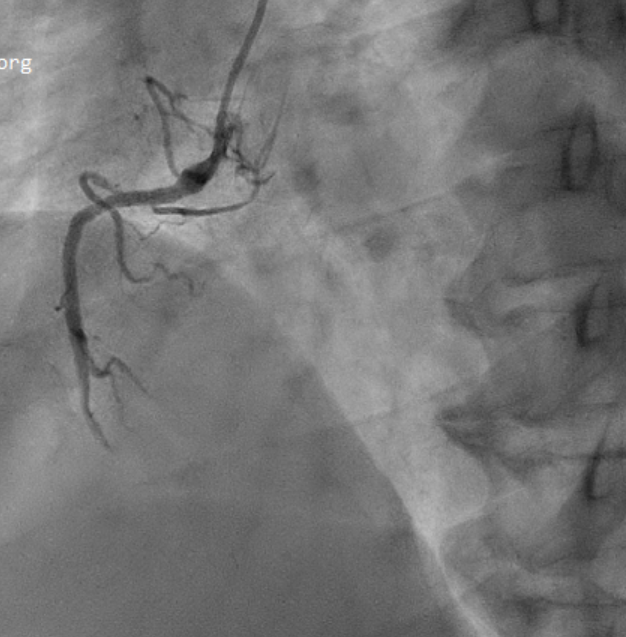
Primary percutaneous coronary intervention (PCI) via right radial approach was performed. Angiogram showed triple vessel disease with normal left main stem, proximal left anterior descending artery (LAD) 70-80%, obtuse marginal1 (OM1) Acute total occlusion (ATO) with Thrombolysis in Myocardial Infarction (TIMI) flow of 0, and distal right coronary artery (RCA) ATO with TIMI 0. Thrombus and slow flow were observed proximal to the OM1 and RCA ATO.

Interventional Management
Procedural Step
Started with PCI to RCA. Guiding catheter: AL 0.75/6Fr. Crossed lesion and advanced wire Runthrough floppy to Posterior descending artery. Pre-dilated distal RCA with a semi-compliance balloon Emerge (Boston Scientific, USA) 2.0x15mm @ 6-14atm. PCI to distal RCA with Drug-eluting stents (DES) Xience Xpedition (Abbott Laboratories, USA) 2.5x33mm@8atm and post-dilated with non-compliant balloon Trek (Abbott Laboratories, USA) 3.0x12mm@16-18atm.
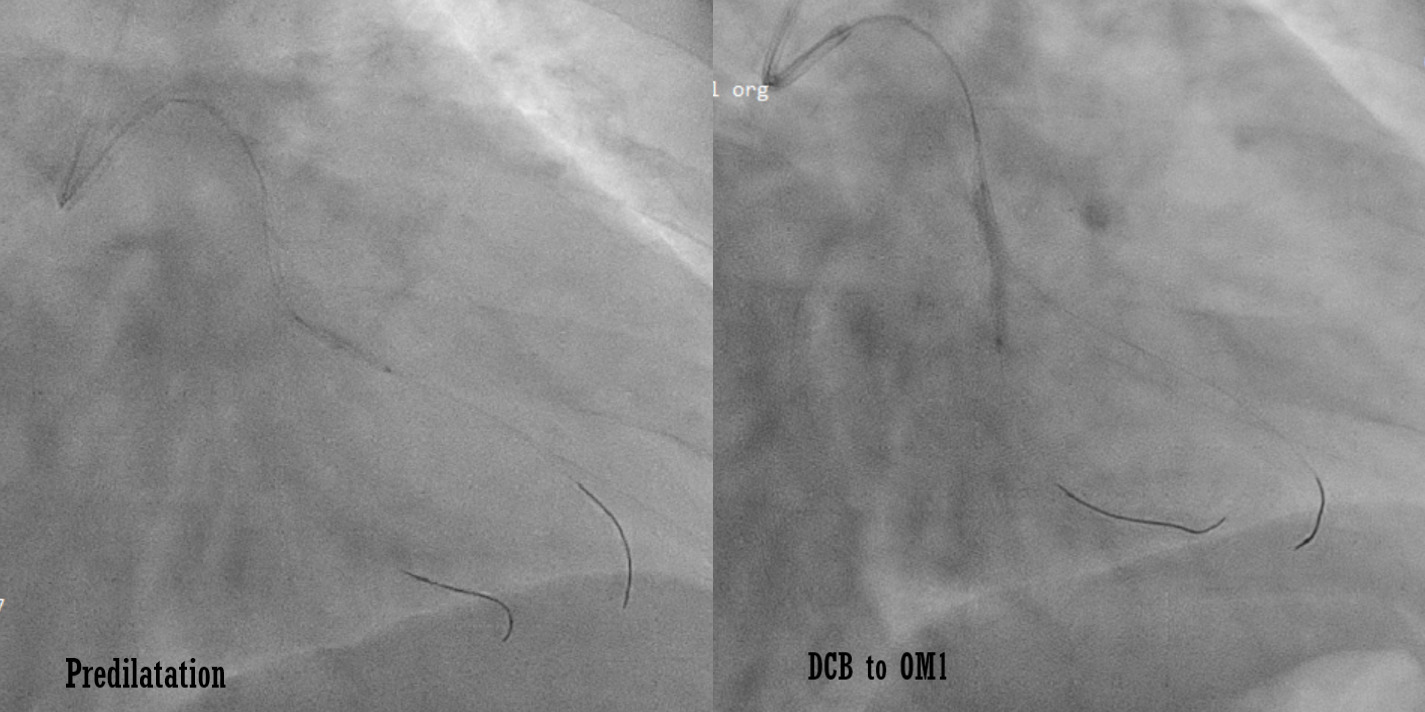
Subsequently proceeded with PCI to LCX. Guiding catheter: XB 3.0/6Fr. Crossed lesion and advanced wire Runthrough floppy to OM1. Pre-dilated OM1 with a semi-compliance balloon Emerge (Boston Scientific, USA) 2.0x15mm@6-12atm. Second Runthrough floppy was advanced to OM’s branch and predilated with semi-compliance balloon Emerge (Boston Scientific, USA) 2.0x15mm @6-8atm. PCI to OM1 with SeQuent Please NEO (B. Braun, Germany) 2.5x20mm@7atm x 60seconds.
Successful PCI with DES at RCA and DCB at OM1 were performed. Achieved good result with TIMI III flow at RCA and OM1. No immediate complications. He was subsequently discharged well with dual antiplatelet therapy, atorvastatin and planned for staged PCI to LAD.


Case Summary
Acute STEMI is usually caused by disruption of the vulnerable atheromatous plaque, leading to thrombus and subsequently total occlusion of a single vessel. Simultaneous multi vessels acute total occlusion is uncommon but can be potentially fatal. It is important for physician to recognize this phenomenon. Timely and careful examination of all the coronary arteries during angiogram is important to ensure the appropriate revascularization and to prevent possible serious complications.