
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-121
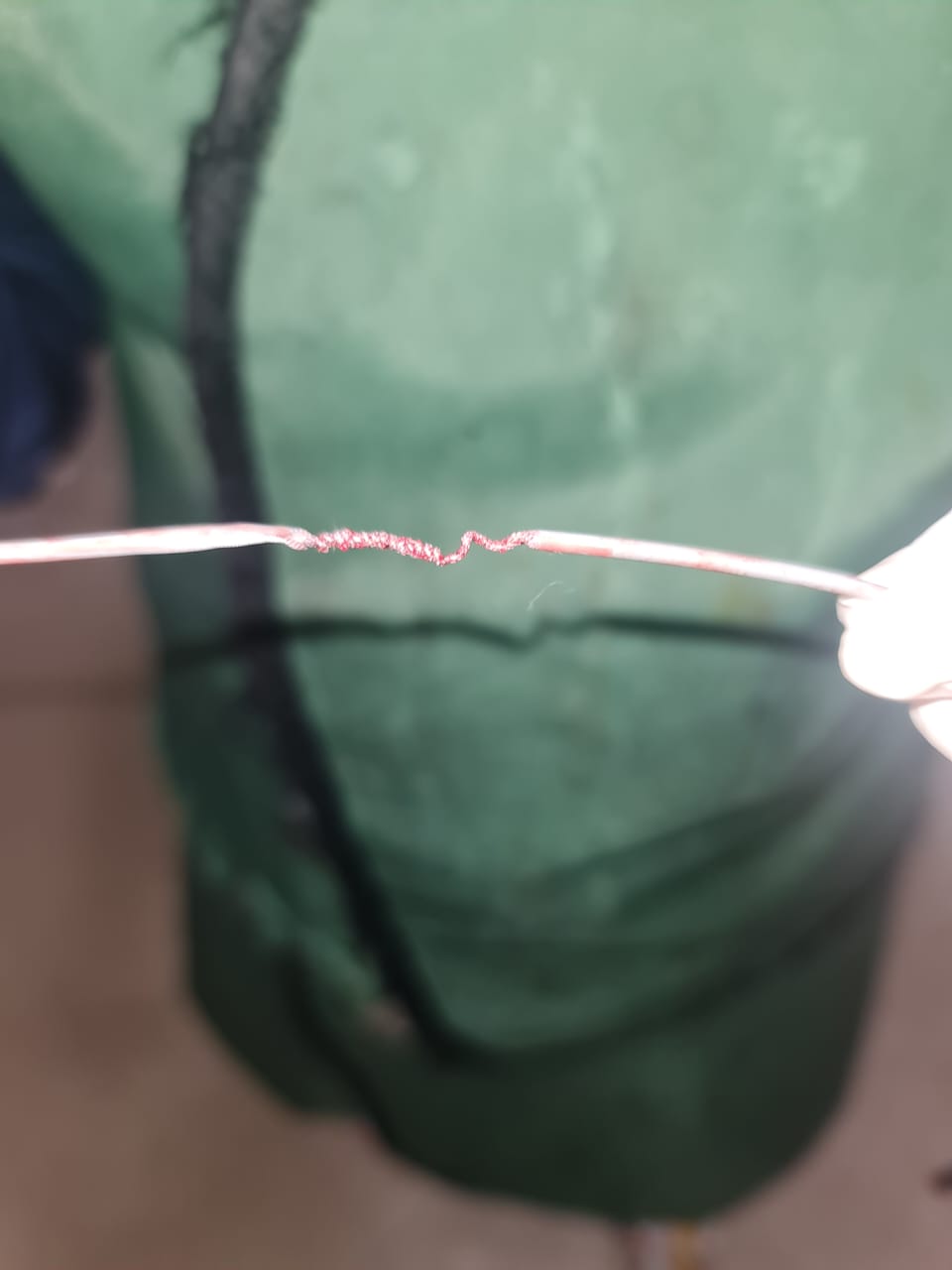
Unraveling the Mysteries of Kinked Coronary Catheters: A Case Series on Troubleshooting in Different Approaches in Limited Resources
By Nikhen Noverike
Presenter
Nikhen Noverike
Authors
Nikhen Noverike1
Affiliation
Universitas Brawijaya - Saiful Anwar General Hospital, Indonesia1,
View Study Report
TCTAP C-121
Coronary - Complication Management
Unraveling the Mysteries of Kinked Coronary Catheters: A Case Series on Troubleshooting in Different Approaches in Limited Resources
Nikhen Noverike1
Universitas Brawijaya - Saiful Anwar General Hospital, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Case 1 A 77-year-old malewith risk factors of hypertension, an active smoker, and a history of acutecoronary syndrome a month ago, still developed symptoms of exertional anginaand dyspnoea on effort, Case 2 A 67-years old malewith risk factors of hypertension and a history of smoking. Physical examination were unremarkable, but from angiography showed in 1st case there were several tortuous in vascular access femoral and also radial


Relevant Test Results Prior to Catheterization
We used gentle maneuver, and also tried multiple guidewire but still unsuccessful. in 2nd case we also tried to sedated patient due to vascular spasm, because of limited resources we used snaring technique for both cases although from different access

Relevant Catheterization Findings
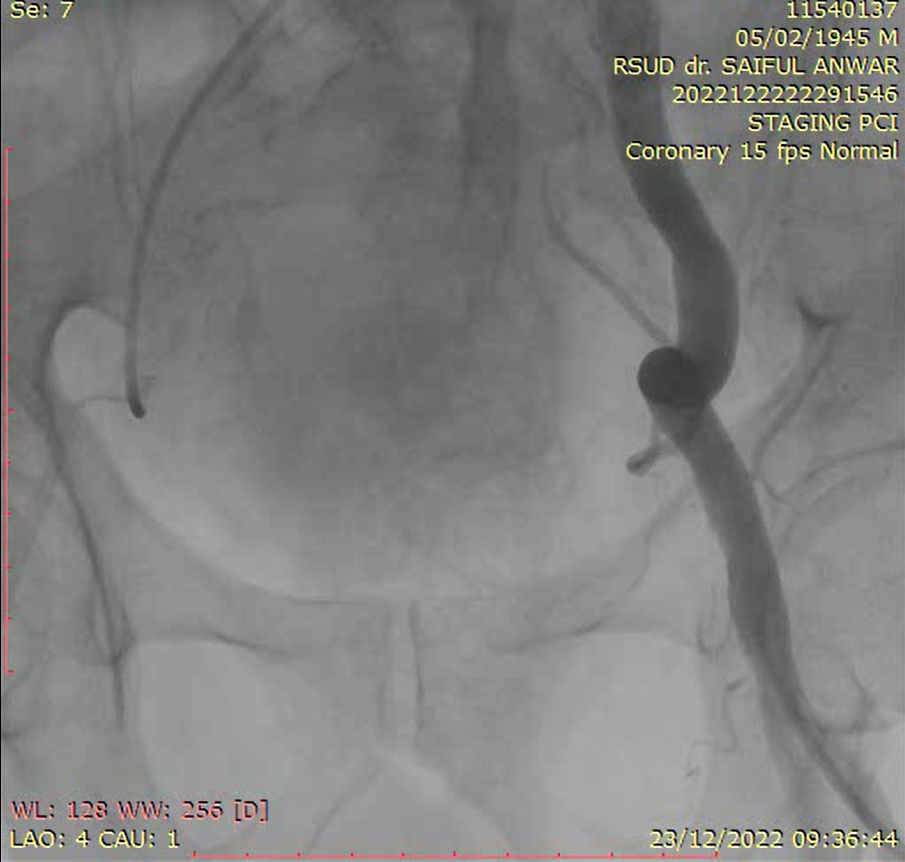
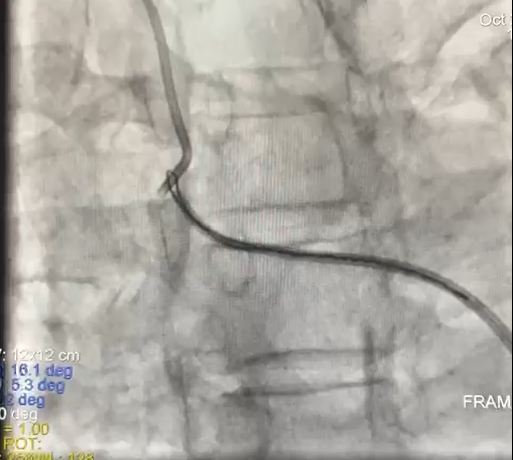
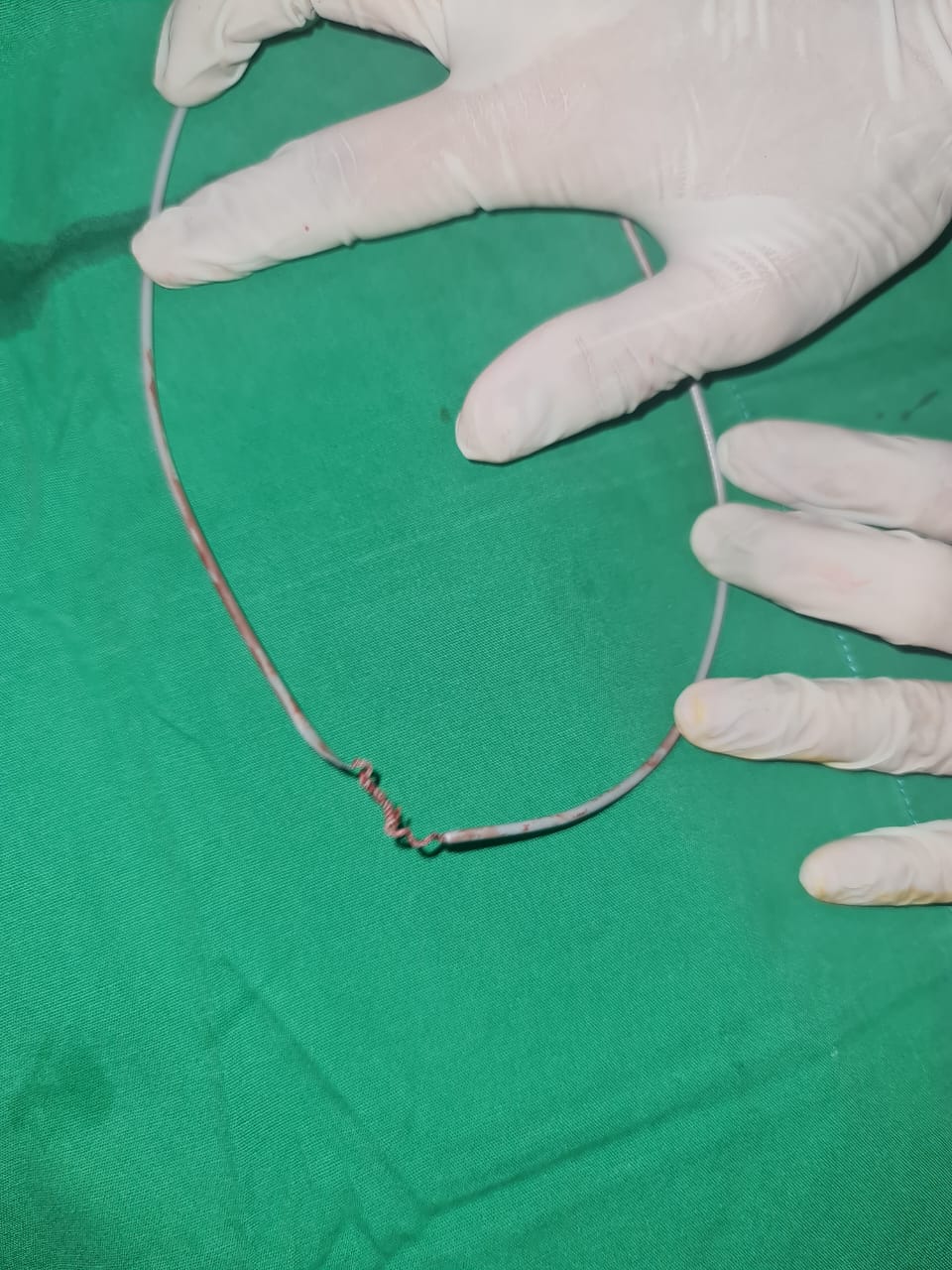
Case 1 kinked catheter at right femoral artery, under fluoroscopy, knotted catheter was pulled out by using snare delivery technique from trans radial access because tortuous at contralateral access. The knotted catheter was pulled out Case 2 Kinked catheter at right antebrachia, Patient sedated. Catching the tip with snare from trans femoral access. Twisted catheter successfully removed.
Interventional Management
Procedural Step
Case 1coronary angiography through trans femoral, showed severe tortuous at the right iliac artery and severe knotted of the guide catheter. Because of the significant tortuosity of the vasculature, even a gentle opposite rotation maneuver and the antegrade advancement of multiple guidewires failed to untwist the guide catheter. Due to left iliac artery was tortuous we decided to use the right trans-radial approach although showed tortuous at the right subclavian artery. We used a snare catheter 15mm, from the proximal tip of the knotted catheter was pulled up into the subclavian artery. To ensure the catheter tip was securely fastened, we rotated it gently after knotting it. At last, we untangled and pulled it out of the right femoral vein. No vascular problems were seen. We resumed percutaneous coronary intervention (PCI) through the left femoral artery, which was completed successfully. Case 2During fluoroscopy, an evaluation showed catheter entrapment of the antebrachial artery. We did a gentle opposite rotation maneuver to retrieve the catheter. Due to limited resources, we sedated patient and decided to use a transfemoral approach by the 7-French sheath and snared from the proximal tip of the knotted catheter with gentle rotation to the knotted catheter, confirming fixation of the catheter tip. Then we straightened and retrieved the catheter from the right trans radial access. We evaluated from angiography that there were no further complications

Case Summary
In limitedresources, Although it happens infrequently, a knottedcatheter can become entrapped. There are a variety of techniques that can betaken to deal with this difficulty. Our cases show snaring technique to snagthe catheter's tip and untied the loop's knot even though from differentapproaches. Both were discharged without complication. This prevented the needfor unscheduled surgical intervention.