
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-208
A Rare PCI for Right Main Bifurcation
By Po-Hsueh Su
Presenter
Su Po Hsueh
Authors
Po-Hsueh Su1
Affiliation
National Cheng Kung University Hospital, Taiwan1,
View Study Report
TCTAP C-208
Innovation - Technology Trends in Coronary Intervention
A Rare PCI for Right Main Bifurcation
Po-Hsueh Su1
National Cheng Kung University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
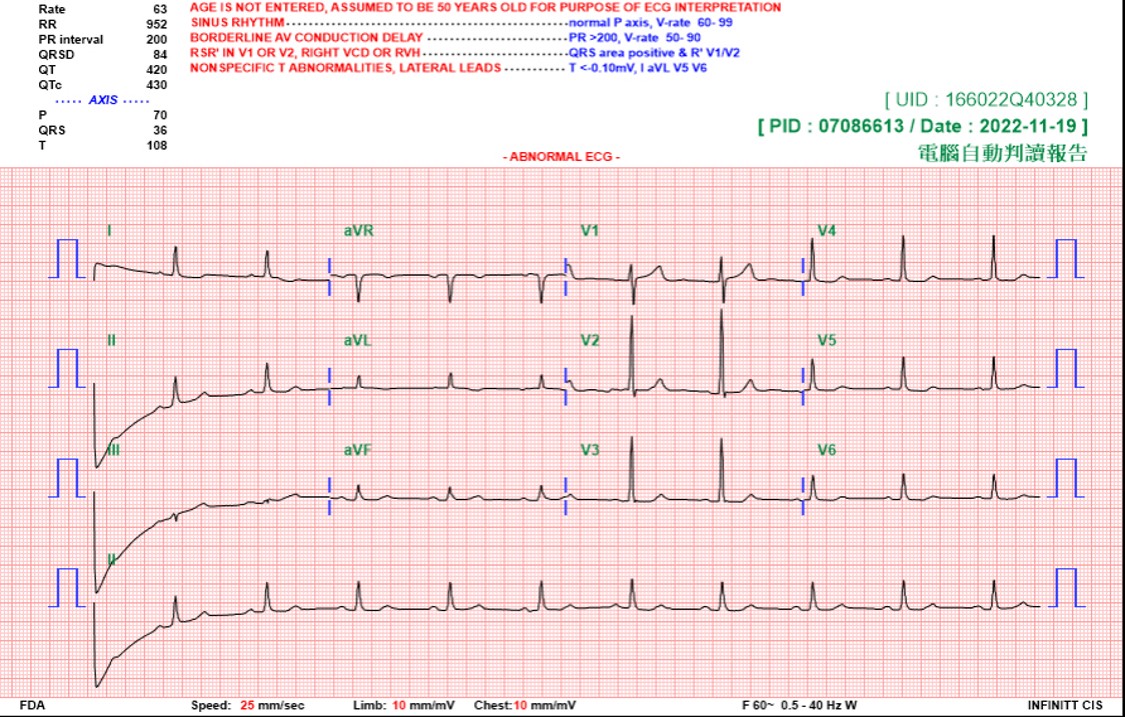
Wepresented the case of a patient with non-ST-elevation myocardial infarctionwith coronary arteries of an anomalous origin, an interarterial course of the LMCA,a unique wide-angle “right” main bifurcation lesion, and a high SYNTAX score. Managementwith contemporary PCI and imaging may be an alternative to surgery.


Relevant Test Results Prior to Catheterization
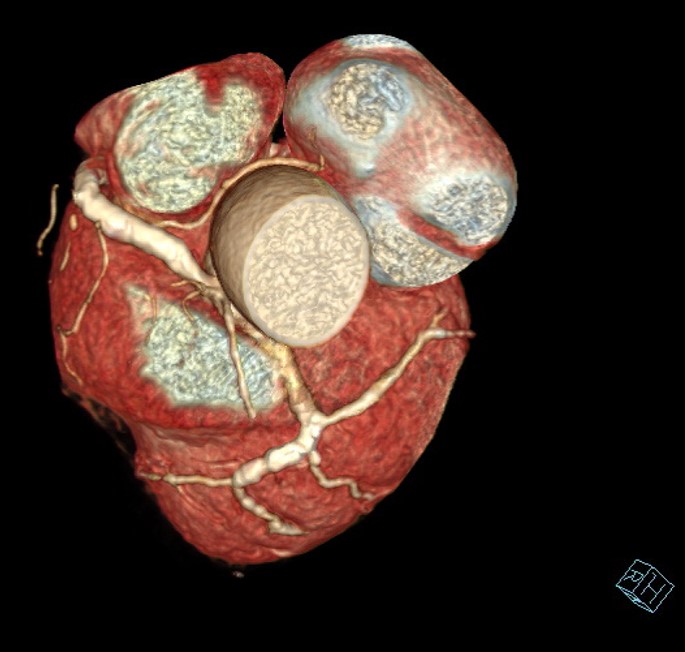
For detailed anatomy, weperformed coronary computed tomography angiography (CCTA), which revealed ananomalous origin of the left main coronary artery (LMCA) from the right sinusof Valsalva and an interarterial course betweenthe aorta and the pulmonary artery; the “right” main bifurcation angle was closeto 180°


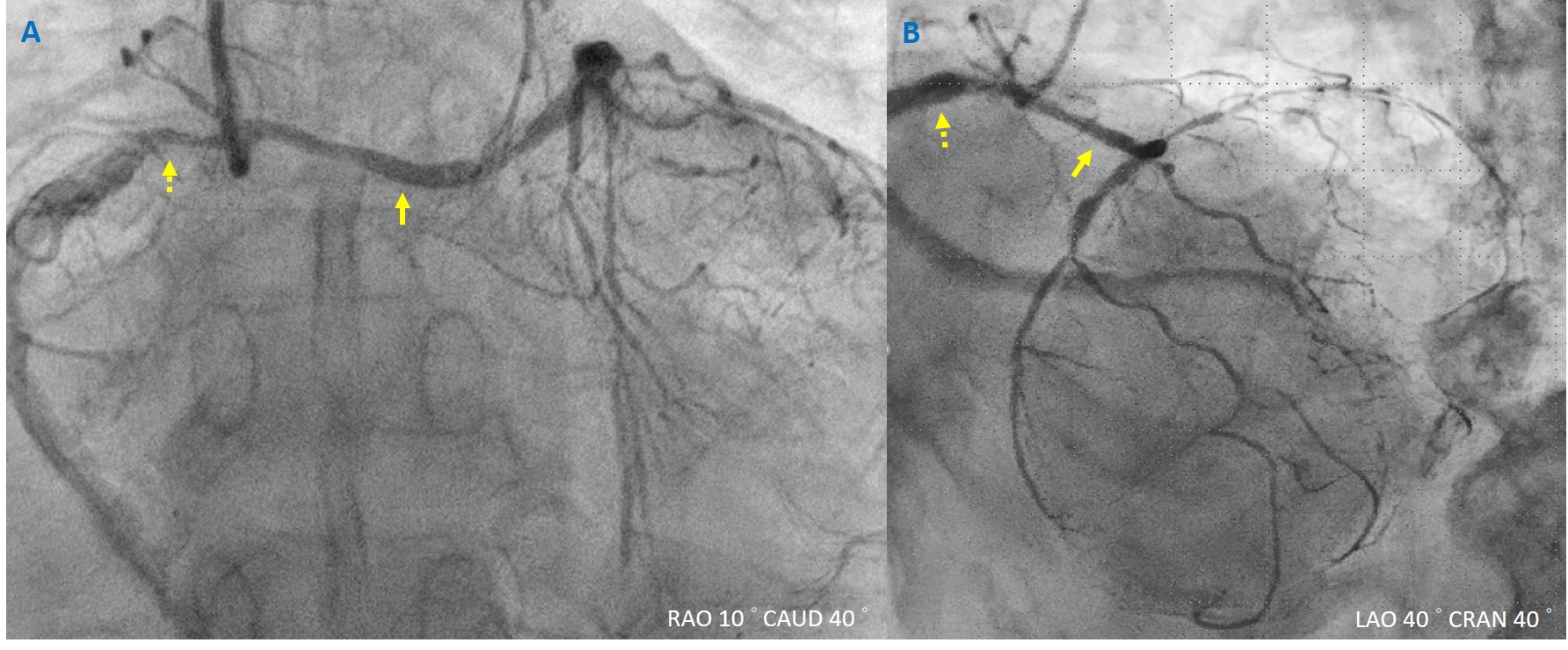
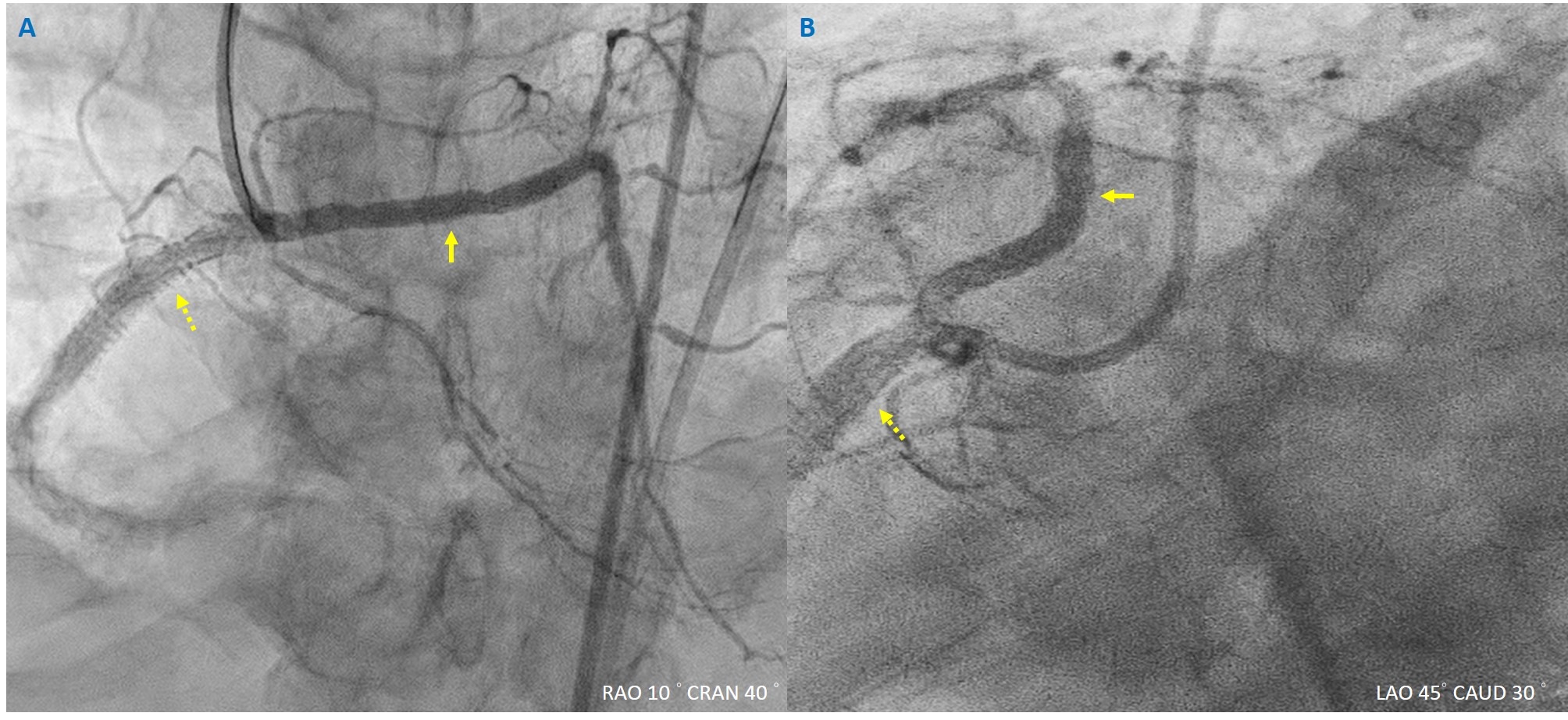
Relevant Catheterization Findings
Our strategy was to perform stenting with little protrusion of the stents into the common ostium. Two guide catheters were used to engage the common ostium. Under the guidance of IVUS and CCTA, the stents were used in both orifices with little protrusion to the common ostium. Afterward, the kissing balloon technique was used to ensure complete stent apposition in both orificesThe IVUS showed that the stents were well apposed without external compression on images.


Interventional Management
Procedural Step
1. A SAL 1 SH 6 Fr. guiding catheter and a JR 4 SH 6 Fr. catheter were used to engage the common orifice.2. The Runthrough NS Hypercoat wire to distal LAD, and the Fielder FC wire to distal RCA. IVUS was then utilized to evaluate vessel condition.3. An Euphora balloon (3.0*15mm) to dilate LM with 8 bars.4. The Sion wire to the intermedius artery.5. An Euphora balloon (2.0*15mm) to dilate intermedius artery with 10 bars.6. A NC Emerge balloon (4.0*15mm) to dilate pRCA with 14 bars.7. A Synergy stent (4.5*24mm) deployed at pRCA.8. A Synergy stent (3.5*38mm) deployed at pLM.9. Kissing ballon technique (KBT) using stent balloons, both inflated at 12 bars.10. Post dilation of the LM stent with a NC Emerge balloon (3.5*15mm) with 12-18 bars and a v with 14 bars.11. Post dilation of the RCA stent with a NC Emerge balloon (5.0*15mm) with 14-16 bars.12. A Synergy stent (5.0*12mm) deployed at RCA orfice-pRCA.13. KBT with a conqueror NC PTCA Balloon/APT balloon (3.0*15mm) inflated at the LM stent at 12 bars and a NC Emerge balloon (5.0*15mm) inflated at the RCA stent at 12 bars simultaneously.14. Post dilation of the RCA stent with a NC Emerge balloon (5.0*15mm) inflated at 16 bars and a NC Emerge balloon (5.0*12mm) at 24 bars.15. Final KBT with a NC Emerge balloon (4.0*15mm) inflated at 12 bars at the LM stent and a NC Emerge balloon (5.0*12mm) inflated at 18 bars at the RCA stent.

Case Summary
Wepresented the case of a patient with non-ST-elevation myocardial infarctionwith coronary arteries of an anomalous origin, an interarterial course of the LMCA,a unique wide-angle “right” main bifurcation lesion, and a high SYNTAX score. Managementwith contemporary PCI and imaging may be an alternative to surgery.
|
Mohammad Shafiqur Rahman Patwary (NATIONAL INSTITUTE OF CARDIOVASCULAR DISEASES) Apr 25, 2024
|
|
| Well done and rare case. | |