
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-103
Rota Burr Stall in an Under Expanded Stent
By Vijin Joseph V. F, Rony Mathew, Jabir Abdullakutty
Presenter
VIJIN JOSEPH V. F
Authors
Vijin Joseph V. F1, Rony Mathew1, Jabir Abdullakutty1
Affiliation
Lisie heart Institute, India1,
View Study Report
TCTAP C-103
Coronary - Complication Management
Rota Burr Stall in an Under Expanded Stent
Vijin Joseph V. F1, Rony Mathew1, Jabir Abdullakutty1
Lisie heart Institute, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 63 year old male chronic smoker presented with effort angina class II and postprandial angina since 2 months. He also had history of systemic hypertension since 10 years for which he was non-compliance to hypertensive drugs
Relevant Test Results Prior to Catheterization
His electrocardiogram showed sinus rhythm with no significant ST/T changes. 2 D echocardiography showed no regional wall motion abnormality and normal left ventricular systolic function. He underwent treadmill test which was positive for inducible ischemia at 7. 1 METS. His hemoglobin was 14.3 gm%, creatinine was 1.0 mg/dl and LDL was 180 mg/dl.
Relevant Catheterization Findings
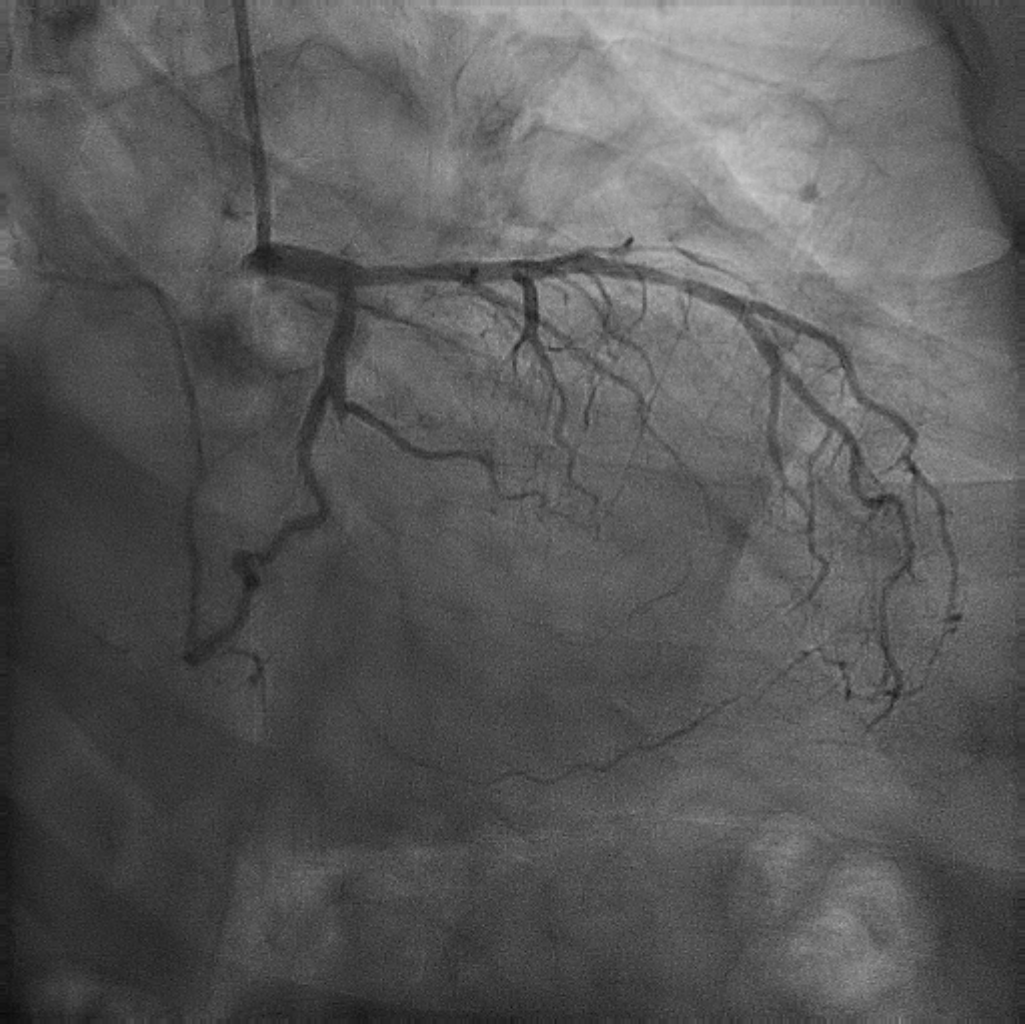
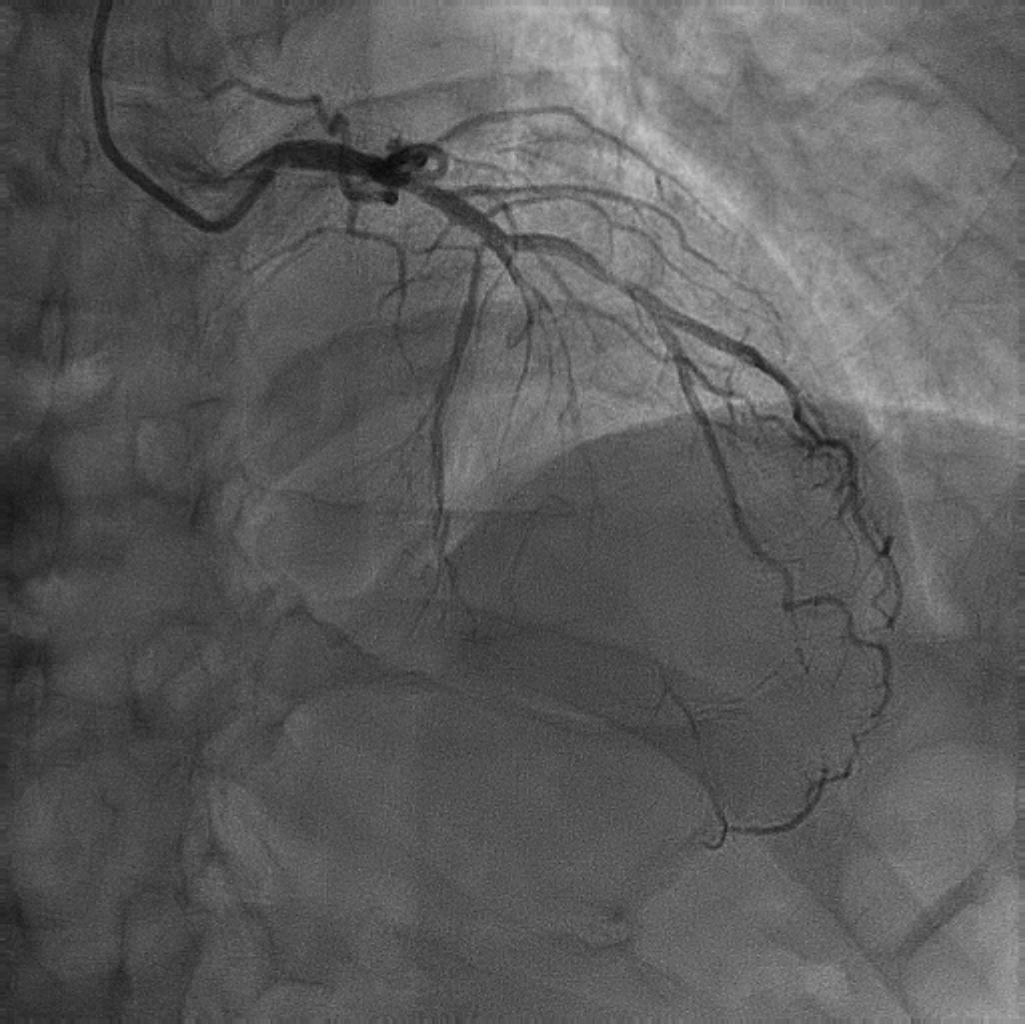
An angiogram revealed a type III LAD vessel with near total occlusion from mid LAD after a good sized diagonal. Diagonal 3 is 2.75mm vessel and proximally it has 60% lesion. LCx was non dominant and normal. OM 1 was totally occluded from proximal part with retrograde filling from LAD. RCA was dominant vessel with mid RCA has 70% lesion and mild calcium. PDA and PLV was normal.
Interventional Management
Procedural Step
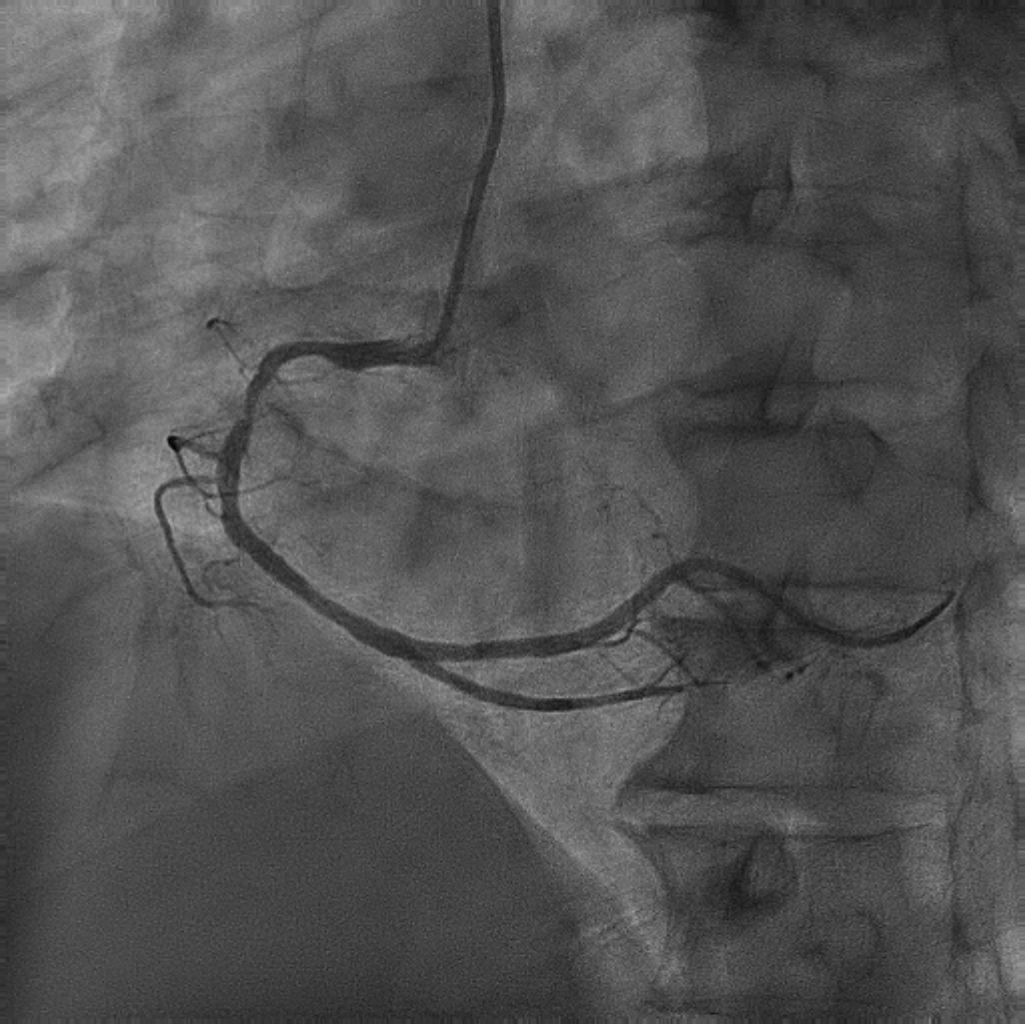
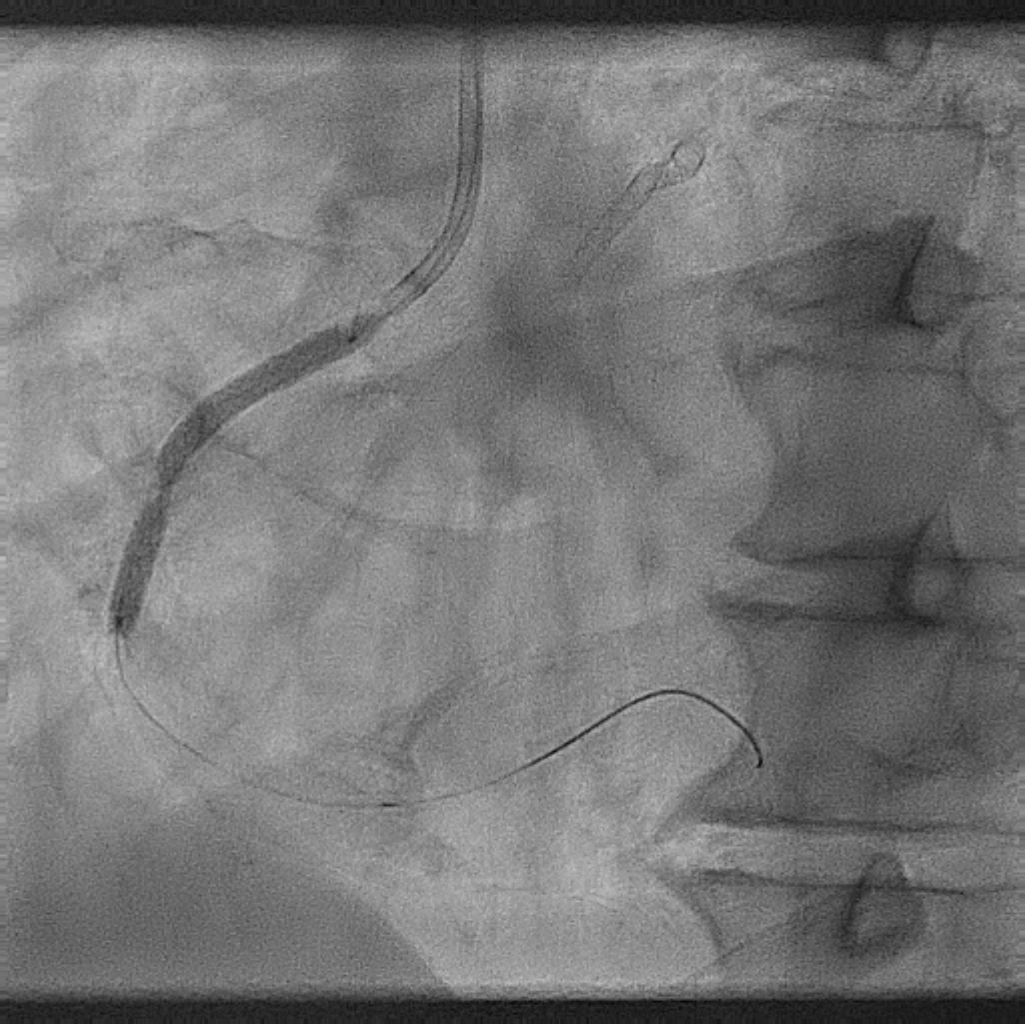
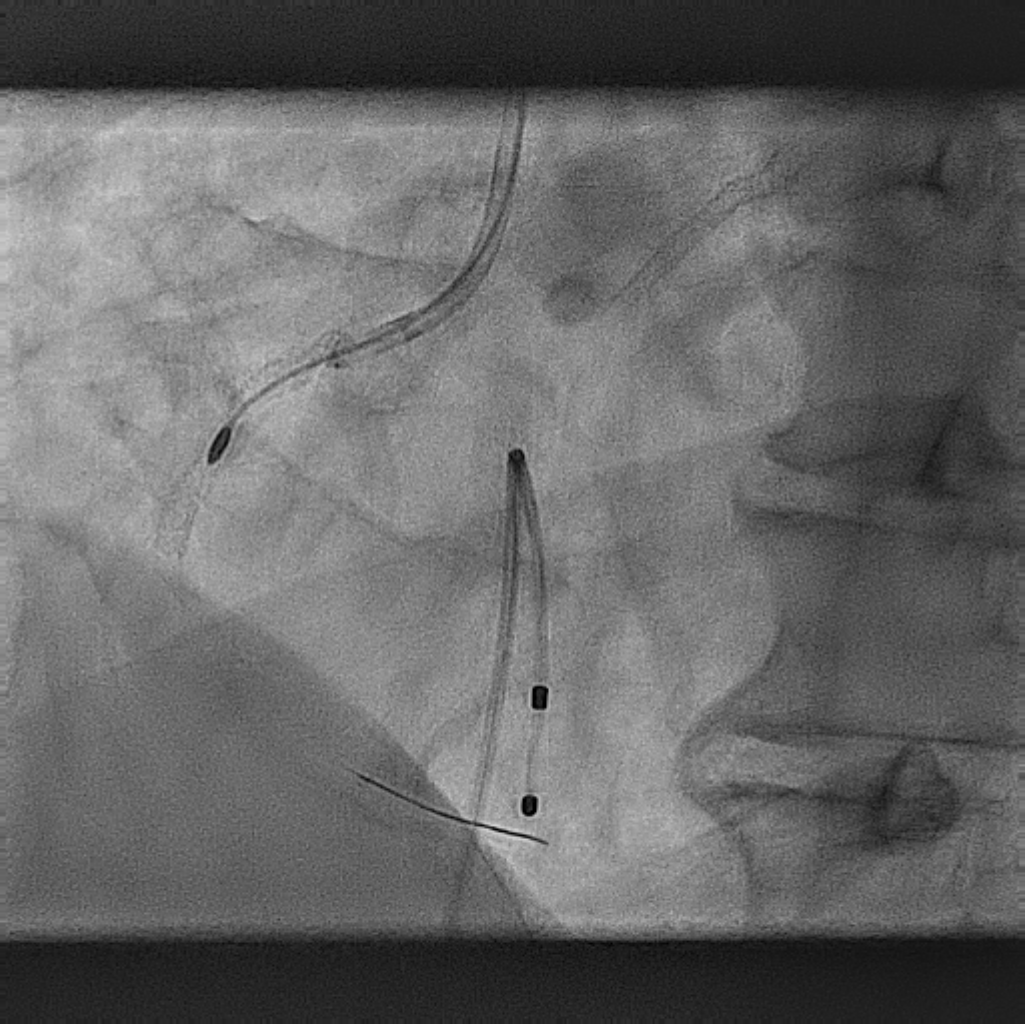
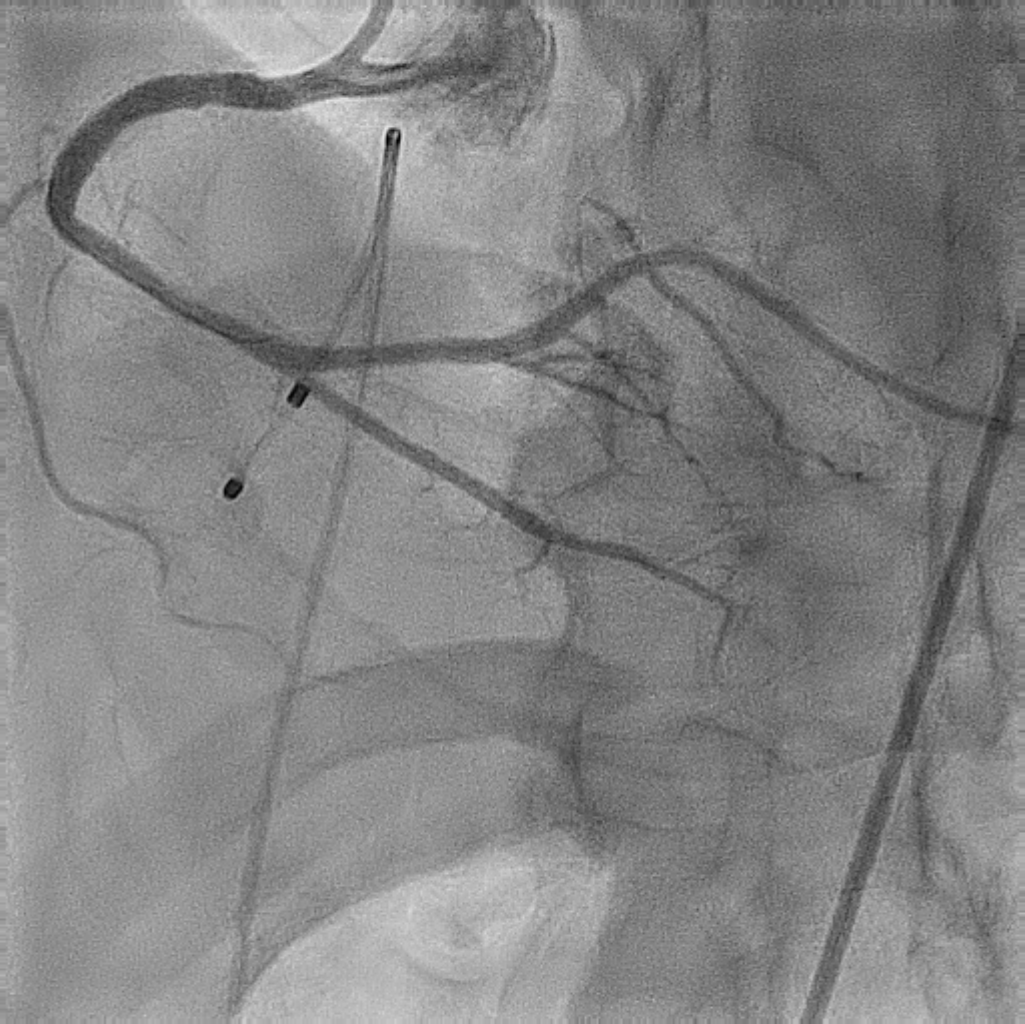
Initially the LMCA was cannulated with 7F EBU 3.5 guiding catheter and the mid LAD lesion and OM 1 lesion was crossed with Fielder XT A wire and subsequently stented with 2.75 x 38mm and 2.5 x 28mm drug eluting stent and post dilated both the lesions with non-compliant balloon at high pressures. Then the RCA was cannulated with 7F JR 3.5 guiding catheter and crossed the lesion with BMW wire. The lesion was stented with 3 x 38mm drug eluting stent without predilation. Post stenting there was dog bone effect, hence attempted to post dilate with non-compliant and high pressure balloons, but the lesion was not yielded due to significant calcium. Hence attempted to do rotational atherectomy with 1.5mm BURR, but unfortunately the Rota burr stalled in mid RCA. Multiple attempts to retrieve the burr by progressing the guide extension catheter over the rota wire failed. Finally the rota burr retrieved by the traction of 5F multipurpose catheter. The underexpanded lesion was then crossed with OPN balloon through guide extension catheter and the lesion was cracked at 30 atm. An OCT showed circumferential calcium with stent fracture in the mid RCA and longitudinal stent deformation in the proximal part. The mid RCA was then stented with 3.5 x 16mm drug eluting stent and post dilated with non-compliant balloon at high pressures. Final OCT showed MSA of 6.3sqmm in mid RCA.
Case Summary
Angiographically the calcium will not be visible well, so always predilate the lesion before stenting. An intravascular imaging helps to determine the length and depth of calcium before stenting, so that if there is significant calcium we can do adequate calcium modification prior to stenting.