
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-209
Emergency Transcatheter Aortic Valve Implantation Under Extracorporeal Membrane Oxygenation for Cardiogenic Shock due to a Bicuspid Aortic Stenosis With Large Annulus
By Shinnosuke Nomura, Shuhei Tsuji, Junichi Tazaki, Mamoru Toyofuku
Presenter
Shinnosuke Nomura
Authors
Shinnosuke Nomura1, Shuhei Tsuji1, Junichi Tazaki1, Mamoru Toyofuku1
Affiliation
Japanese Red Cross Wakayama Medical Center, Japan1,
View Study Report
TCTAP C-209
Structural - Aortic Valve Intervention - Bicuspid AV
Emergency Transcatheter Aortic Valve Implantation Under Extracorporeal Membrane Oxygenation for Cardiogenic Shock due to a Bicuspid Aortic Stenosis With Large Annulus
Shinnosuke Nomura1, Shuhei Tsuji1, Junichi Tazaki1, Mamoru Toyofuku1
Japanese Red Cross Wakayama Medical Center, Japan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 79-year-old man was diagnosed severe aortic stenosis (AS) and aortic regurgitation (AR) of a bicuspid aortic valve 6 years ago, however, he had refused surgical aortic valve replacement because he didn’t have any symptoms. He was admitted to previous hospital with dyspnea and leg edema. His symptoms were not improved for two weeks after treatment for heart failure. He was transferred to our hospital for additional invasive treatment. He presented symptoms of cardiogenic shock.
Relevant Test Results Prior to Catheterization
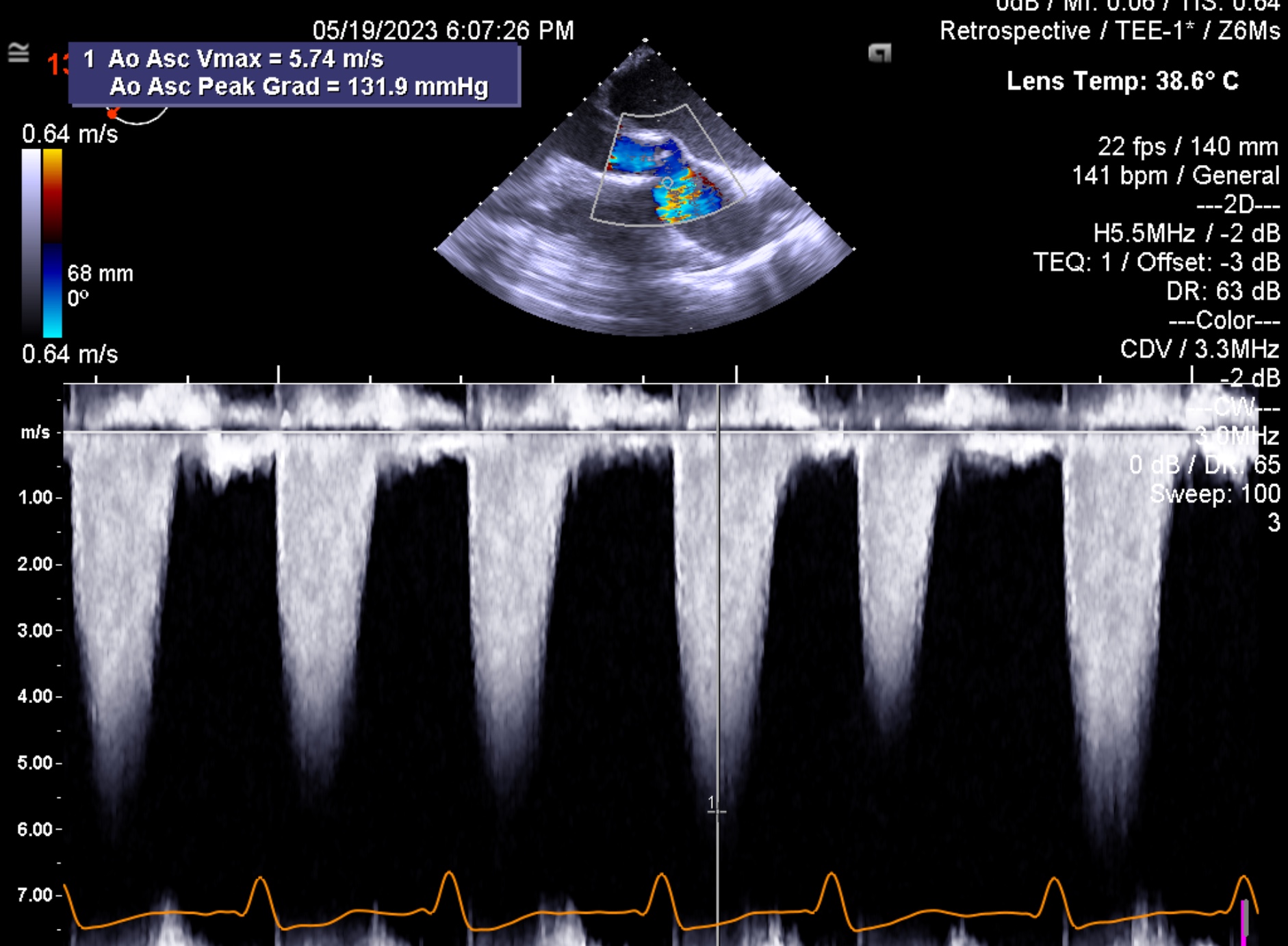
Echocardiography revealed poor LV function with low ejection fraction (LVEF) 25%, left ventricular end-diastolic dimension (LVDd) were dilated to 72mm. Peak systolic velocity of aortic valve was 4.6m/s with severe AR. Coronary angiography showed no organic stenosis. Cardiac computed tomography (CCT) confirmed a calcified bicuspid aortic valve. The area of annulus was 700-730mm2 and perimeter of annulus was 100-110mm.
Relevant Catheterization Findings
None
Interventional Management
Procedural Step
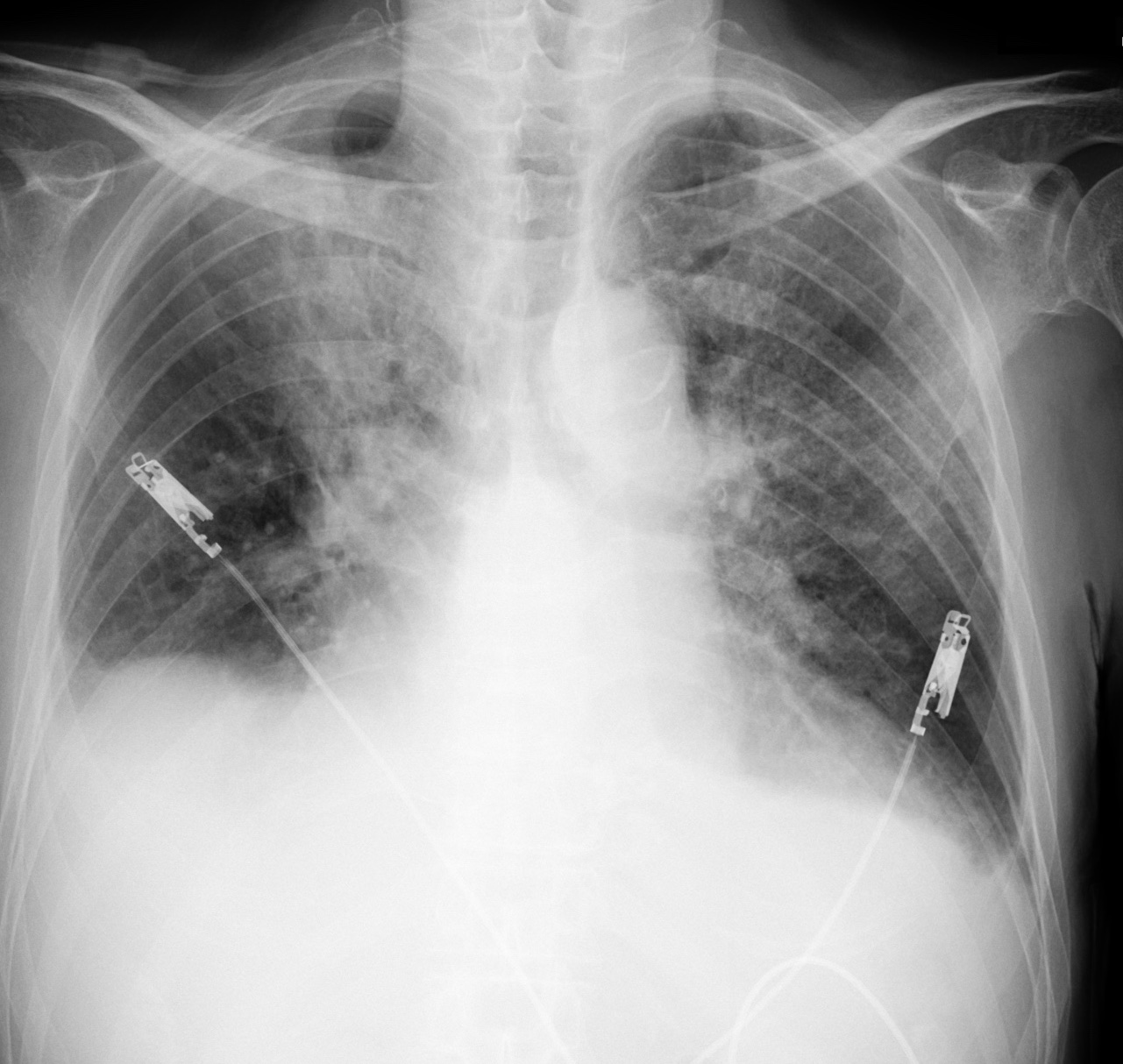
Intubation and intra-aortic balloon pumping (IABP) were started at his right femoral artery. However hemodynamic states was not stabilized. We thought the invasive treatment for severe AS/AR is necessary to improve his clinical status. The patient’s large annulus was beyond the recommendation range of Sapien3 29mm valve (Edwards Lifesciences, Irvine, CA, USA), which is largest size in Japan. However, the risk of surgical valve replacement was extremely high (Euro score II: mortality32.9%, STS score: 17.4%). After the careful discussion, our heart team decided to perform transfemoral transcatheter aortic valve implantation (TAVI) with the Sapien3 29mm valve. Emergent TAVI procedure was performed under general anesthesia with transesophageal echocardiography. At first V-A extracorporeal membranous oxygenation (ECMO) was installed from his left femoral artery/vein to maintain hemodynamic stability during TAVI procedure. The IABP at his right femoral artery was replaced with a 16Fr E-sheath (Edwards Lifesciences, Irvine, CA, USA).The Sapien3 29mm valve was prepared with 1ml overfilling (34ml). After deployment, Echocardiography revealed mild-moderate paravalvular leak (PVL) due to incomplete device attachment to annulus. Therefore, we decided to perform post dilation with 2ml overfilling (35ml). After additional dilation, echocardiography showed reduced PVL and optimal frame expansion. The Aorta-LV pressure gradient reduced to 10mmHg.


Case Summary
His clinical status improved gradually, and then V-A ECMO was removed on the next day after TAVI. He was discharged from CCU on Day15. The patient finally returned home on Day 59.At the postoperative 3 months follow‐up, the patient remained in good condition. Echocardiography revealed minimal PVL, LVEF increased to 44%, reduction of LVDd to 49mm, and peak systolic velocity of 1.5m/s. The patient was not rehospitalized due to heart failure until now to date.We report a case of successful emergency TAVI for bicuspid aortic valve with severe ASR and large aortic annulus.