
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-011
Paradoxical Coronary Artery Embolism With Decreased Protein C Activity.
By Kota Fujihara, Yohei Oishi, Kenta Uemura, Yuzo Akita
Presenter
Kota Fujihara
Authors
Kota Fujihara1, Yohei Oishi1, Kenta Uemura1, Yuzo Akita1
Affiliation
Osaka Saiseikai Izuo Hospital, Japan1,
View Study Report
TCTAP C-011
Coronary - ACS/AMI
Paradoxical Coronary Artery Embolism With Decreased Protein C Activity.
Kota Fujihara1, Yohei Oishi1, Kenta Uemura1, Yuzo Akita1
Osaka Saiseikai Izuo Hospital, Japan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
This is 30’s old male without any past history of illness even the Kawasaki disease. He had no family history of ischemic heart disease. His coronary risk factor was smoking only. He came to our hospital on foot for sudden onset of chest pain.

Relevant Test Results Prior to Catheterization
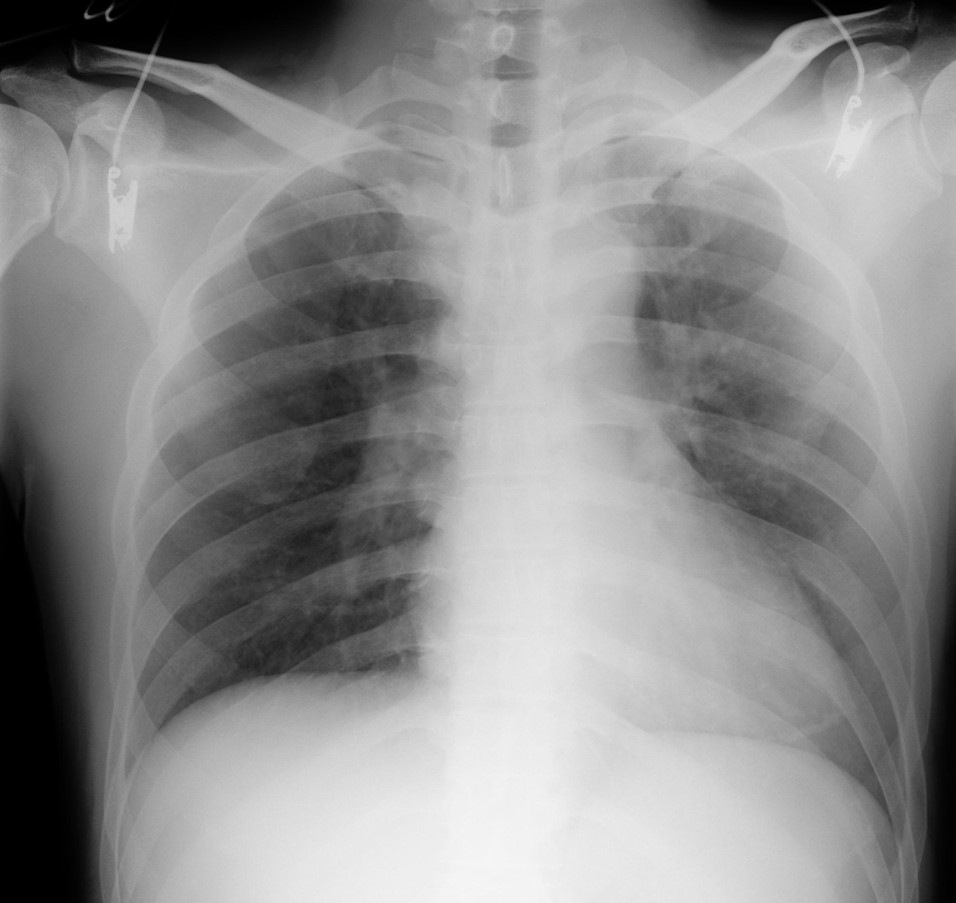
His ECG showed normal sinus rhythm and premature atrial contraction , ST elevation in Ⅱ, Ⅲ, aVF, V4-6. His chest X-ray showed cardiomegaly and lung congestion. His blood test resulted WBC was increased but cardiac enzyme was not elevated at that time.

Relevant Catheterization Findings
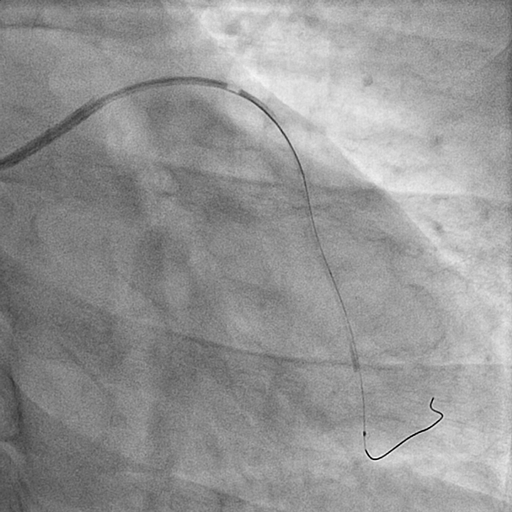
CAG showed there is a big thrombus at proximal LAD, total occlusion in distal LAD.

Interventional Management
Procedural Step
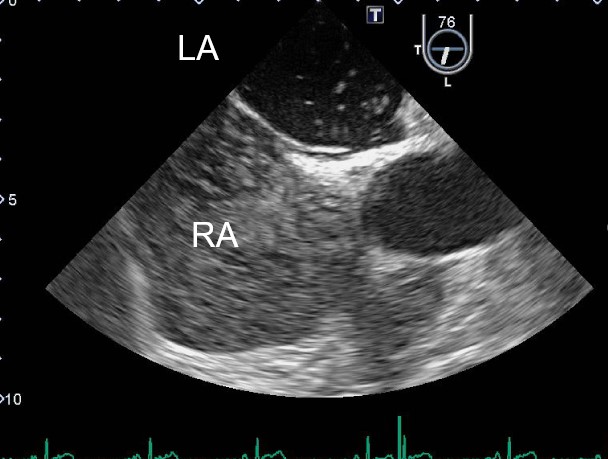
He underwent primary PCI to LAD. We aspirated thrombus by the thrombectomy catheter. We could get TIMI-3 flow after thrombus aspiration, but the thrombus was still existed at the proximal LAD. We finished this procedure because of got TIMI-3 flow.We performed CAG and OCT 3days after primary PCI. His LAD had TIMI-3 flow and the existed thrombus was disappeared from CAG. The OCT image showed a mural thrombus at the proximal LAD without ruptured plaque. His coronary CT also showed mural thrombus at the proximal LAD. We suspected the thrombus came from the extra heart. His protein C activity was decreased by his blood test. His bubble test by the transesophageal echocardiography was positive and grade3. We diagnosed him a paradoxical coronary artery embolism with decreased protein C activity. His OCT findings and coronary CT findings showed the thrombus was organized.

Case Summary
We experienced STEMI in young adult. The cause of this ACS suspected extra heart thrombus. We diagnosed him a paradoxical coronary artery embolism with decreased protein C activity and existed patent foramen ovale.It is important to investigate the cause of ACS especially for a young people to determination of treatment policy.