
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-073
Chronic Total Occlusion Intervention in a Young, Obese Patient With End Stage Renal Disease: Scraping Through by the Skin of Our Knuckles
By Noor Diyana Binti Mohamad Farouk, Hamat Hamdi Che Hassan, Boon Cong Beh, Mohd Asyiq Al-Fard Bin Mohd Raffali, Shawal Faizal Mohamad, Rosli Mohd Ali
Presenter
Noor Diyana Binti Mohamad Farouk
Authors
Noor Diyana Binti Mohamad Farouk1, Hamat Hamdi Che Hassan1, Boon Cong Beh1, Mohd Asyiq Al-Fard Bin Mohd Raffali1, Shawal Faizal Mohamad1, Rosli Mohd Ali2
Affiliation
Hospital Canselor Tuanku Muhriz UKM, Malaysia1, Cardiac Vascular Sentral Kuala Lumpur, Malaysia2,
View Study Report
TCTAP C-073
Coronary - Complex PCI - CTO
Chronic Total Occlusion Intervention in a Young, Obese Patient With End Stage Renal Disease: Scraping Through by the Skin of Our Knuckles
Noor Diyana Binti Mohamad Farouk1, Hamat Hamdi Che Hassan1, Boon Cong Beh1, Mohd Asyiq Al-Fard Bin Mohd Raffali1, Shawal Faizal Mohamad1, Rosli Mohd Ali2
Hospital Canselor Tuanku Muhriz UKM, Malaysia1, Cardiac Vascular Sentral Kuala Lumpur, Malaysia2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
We present a case of a 41 year-old morbidly obese gentleman, with known history of triple vessel disease and mid RCA CTO. He had been counselled previously for coronary artery bypass graft surgery, however he declined and opted instead for high risk, complex, percutaneous coronary intervention. He also has history of hypertension, dyslipidaemia, type II diabetes mellitus, and end stage renal disease on regular haemodialysis. His body mass index is 41kg/m2.

Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
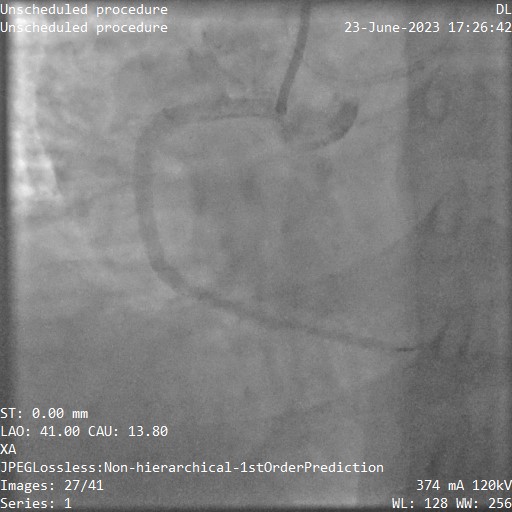
His baseline angiogram showed mild disease in the LMS with severe proximal to mid LAD disease with calcification. The LAD supplies collaterals to the RCA via the septal branches. There is also moderate disease in the mid LCx. The RCA appears dominant, with a CTO at the mid vessel. The distal vessel receives supply from collaterals from the LAD.

Interventional Management
Procedural Step
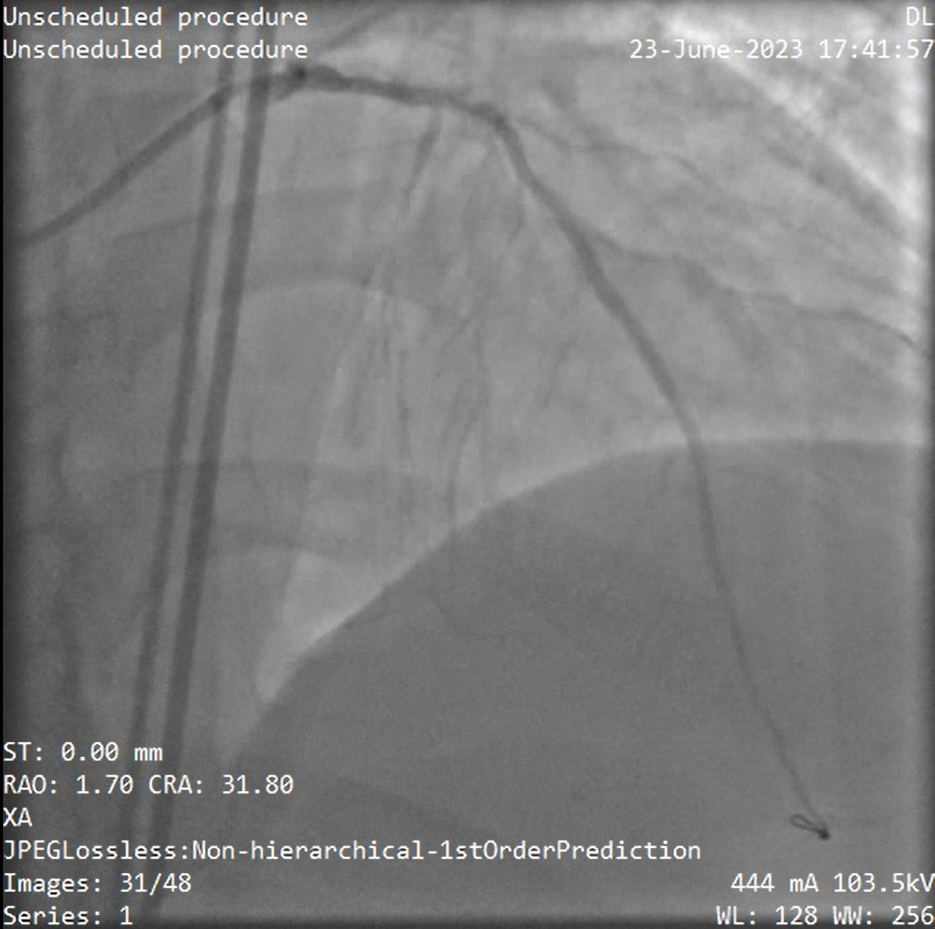
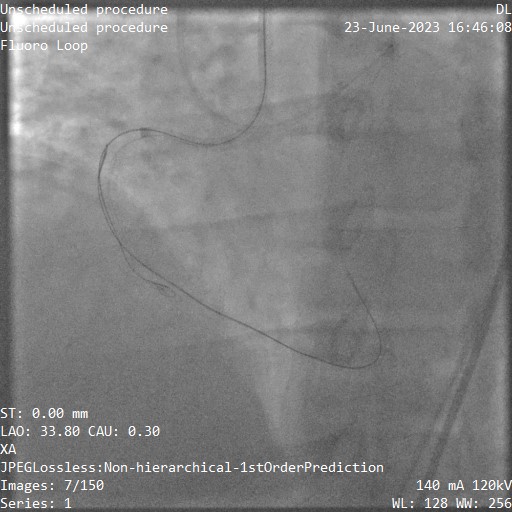
We placed an AL1 catheter in the RCA and a JL4.0 in the LMS through bilateral femoral artery approach. Upon first contrast injection a long dissection of the RCA developed. We switched to an AL0.75 and an EBU3.5. Retrogradely, we advanced a workhorse wire through a microcatheter to the occlusion via the collaterals, then switched to a low tip-load CTO wire. Antegrade contrast injection was kept to a minimum to avoid dissection expansion. Despite using a high tip-load wire, we were unable to cross the CTO. Finally, we used the knuckling technique to penetrate the subintima retrogradely as well as antegrade. Using the dissection created by the antegrade knuckling, we employed the reverse CART method to re-enter the true lumen and an extra-long wire for externalisation. Predilation was done with a 3.0 semi-compliant balloon, then 4.0 non-compliant balloon. The CTO segment was covered using two overlapping stents (3.5 and 4.0) after IVUS assessment. We utilised the Szabo technique to place the stent at the dissected ostium. The stent jutted into the aorta by two struts which we flared at high pressure and the dissection was sealed successfully. Intervention of the LAD was less eventful. Both vessels were intervened at the same sitting to reduce complications from repeat procedures due to his weight. Suture closure devices were unable to penetrate deep enough and were abandoned. Femoral sheaths were replaced and removal using conventional compression method were done the next day.

Case Summary
The ostial dissection was sealed off completely with the placement of the ostial stent. We crossed the long segment CTO using the wire knuckling and modified reverse CART methods. Due to the patient’s body habitus, we were unable to use closure devices. Our attempt was abandoned as the devices were not able to penetrate deep enough to achieve pulsatile backflow. Conventional compression method was used the following day prior to his haemodialysis. Despite this, he still developed a pseudoaneurysm over the left femoral artery. He was referred to interventional radiology for coiling, and has since been discharged well.