
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-025
IVUS-Guided Treatment of Spiral Dissection for Preserving Side Branches
By Yoshinobu Murasato, Kyohei Meno, Takahiro Mori, Katsuhiko Takenaka
Presenter
Yoshinobu Murasato
Authors
Yoshinobu Murasato1, Kyohei Meno1, Takahiro Mori2, Katsuhiko Takenaka2
Affiliation
National Hospital Organization, Kyushu Medical Center, Japan1, Kyushu Medical Center, Japan2,
View Study Report
TCTAP C-025
Coronary - Complex PCI - Bifurcation
IVUS-Guided Treatment of Spiral Dissection for Preserving Side Branches
Yoshinobu Murasato1, Kyohei Meno1, Takahiro Mori2, Katsuhiko Takenaka2
National Hospital Organization, Kyushu Medical Center, Japan1, Kyushu Medical Center, Japan2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
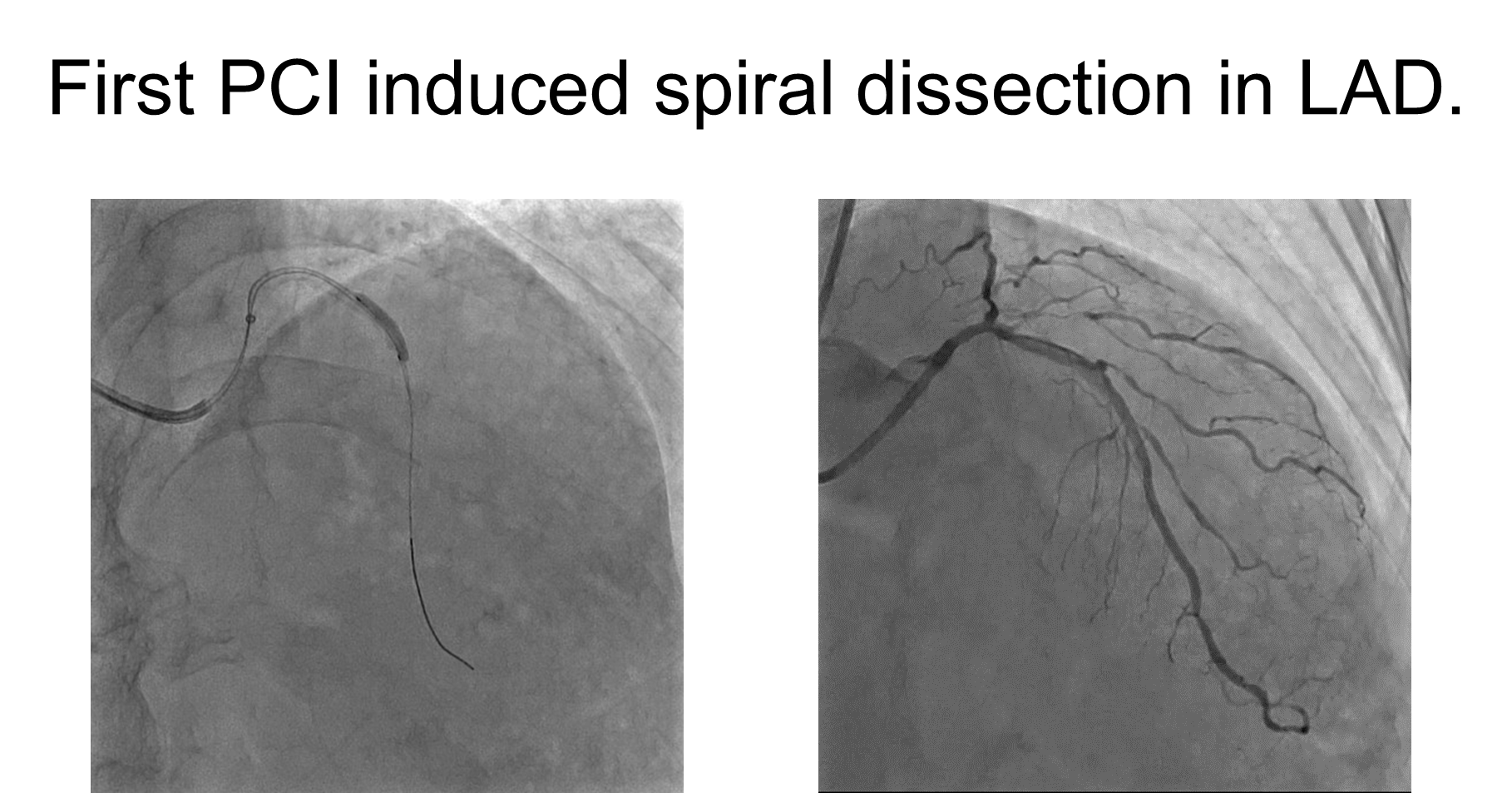
The patient is of a late 60’s male with worsening effort angina in a month. He had a coronary CT in another hospital, demonstrating LAD calcified stenosis, RCA stenosis, and LCX CTO. He underwent CAG and subsequent PCI there. However, they failed to advance a scoring balloon in the calcified LAD and its dilation led to spiral dissection.While coronary flow and ECG remained stable, theyreferred the patient to our hospital for further management.

Relevant Test Results Prior to Catheterization
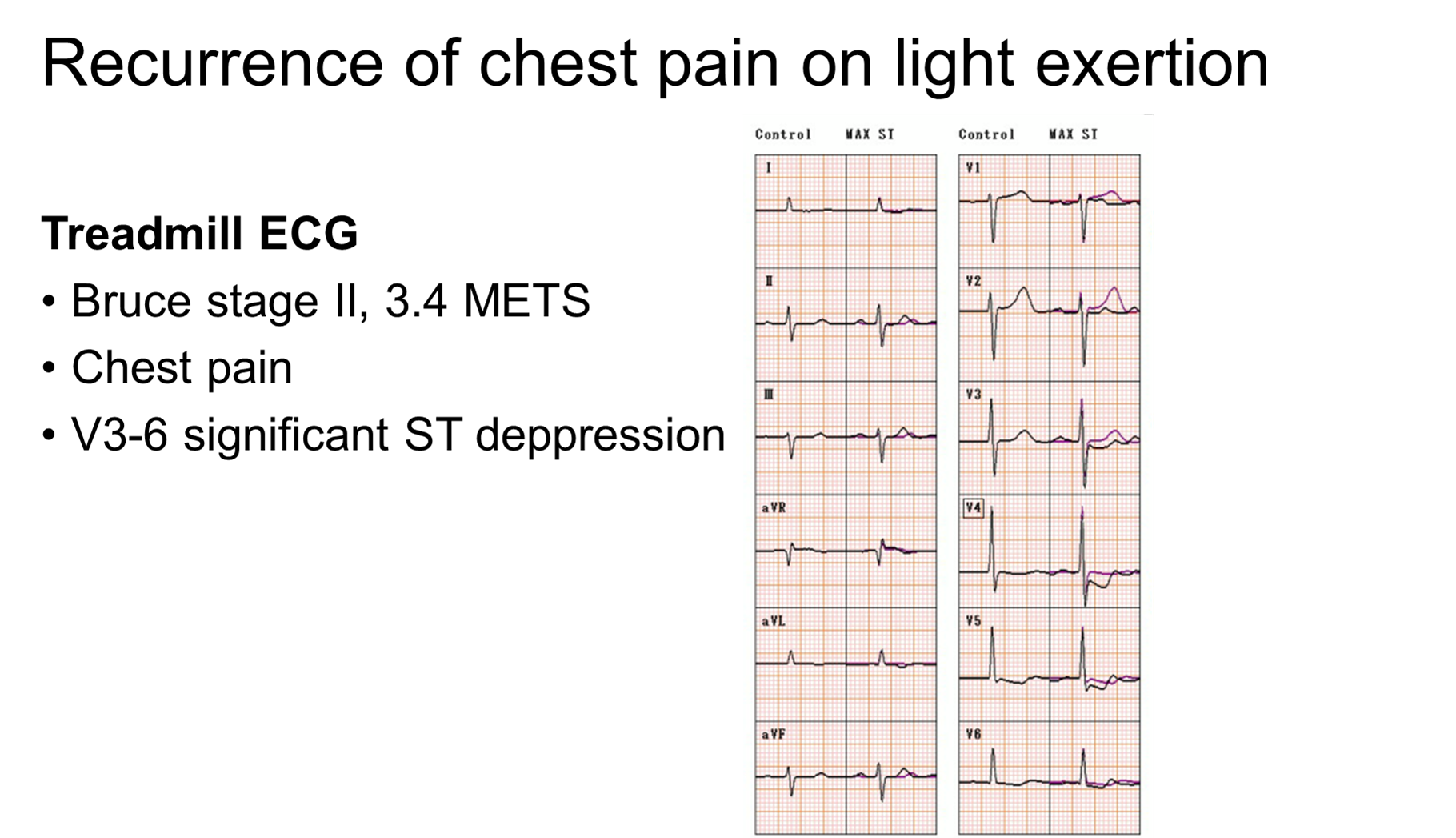
Since there was no significant symptom, ECGchange, or elevation of myocardial enzyme, CAG was performed on the next day, which showed no relevant change in the LAD dissection. A drug-eluting stent was implanted inthe proximal RCA lesion and elective PCI in the LAD was planed after healing the dissection. However, chest pain on light exertion recurrently occurred and treadmill ECG with 3.4METS showed significant ST depression in anterior chest leads.

Relevant Catheterization Findings
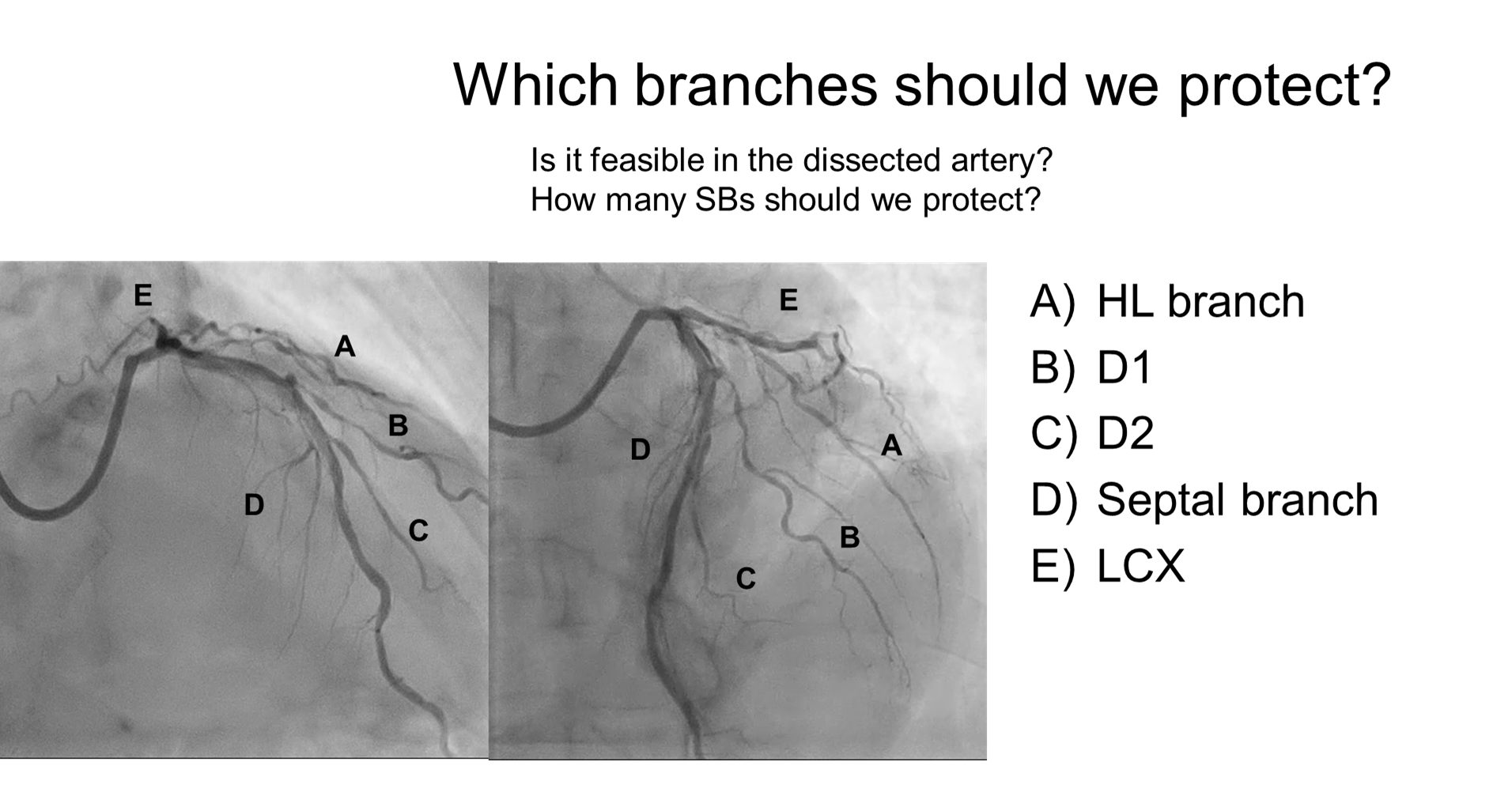
CAG on 7day after first PCI showed the progression of the dissection that narrowed the true lumen in LAD and some narrowing in the left main (LM) coronary artery. There were five major branches derived from the dissected vessel with some luminal narrowing in the ostium, which were LCX, High lateral (HL) branch, first and second diagonal branch, and septal branch. Achieving optimal wiring through the true lumen for each of these branches appeared challenging.

Interventional Management
Procedural Step
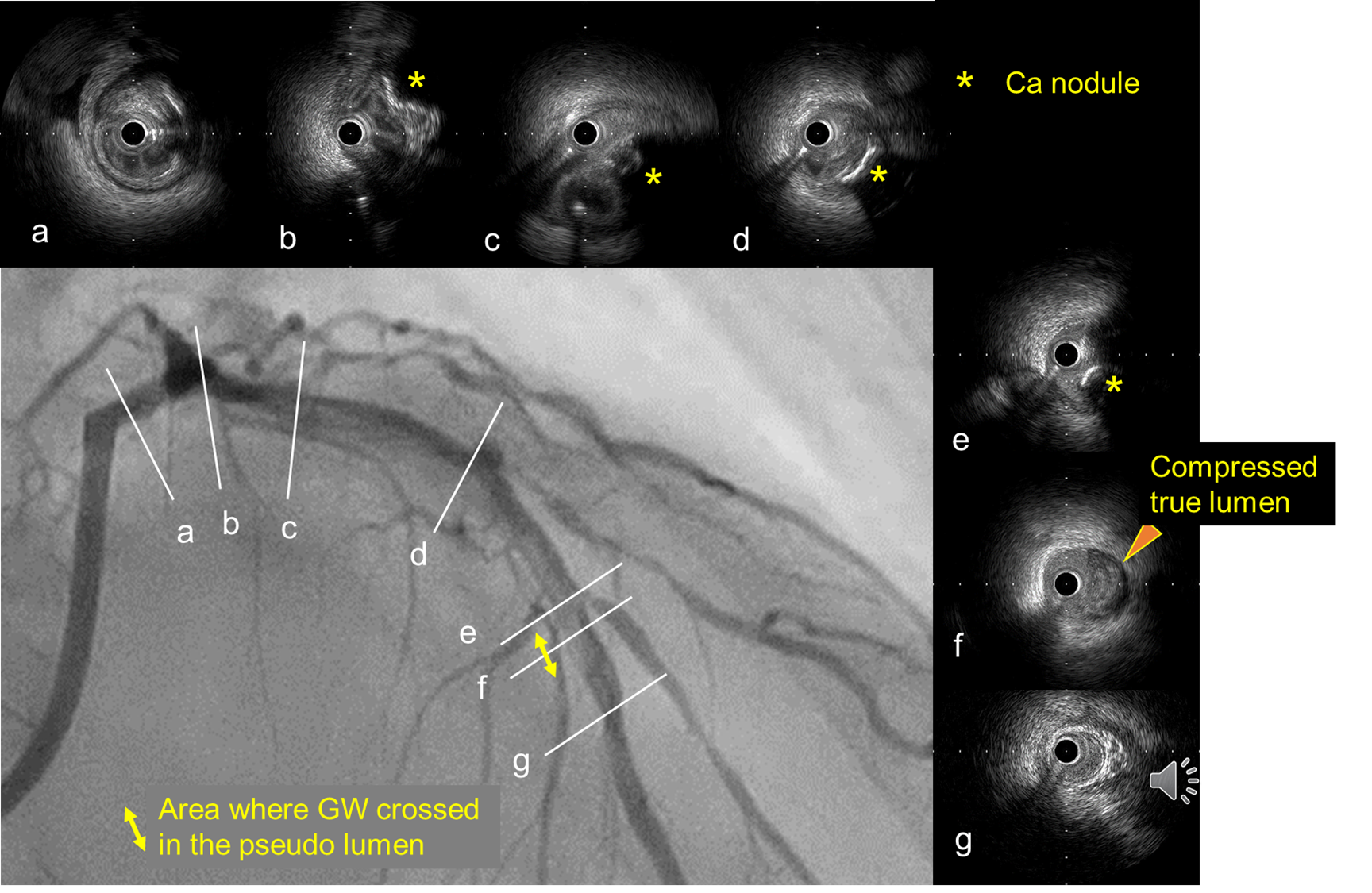
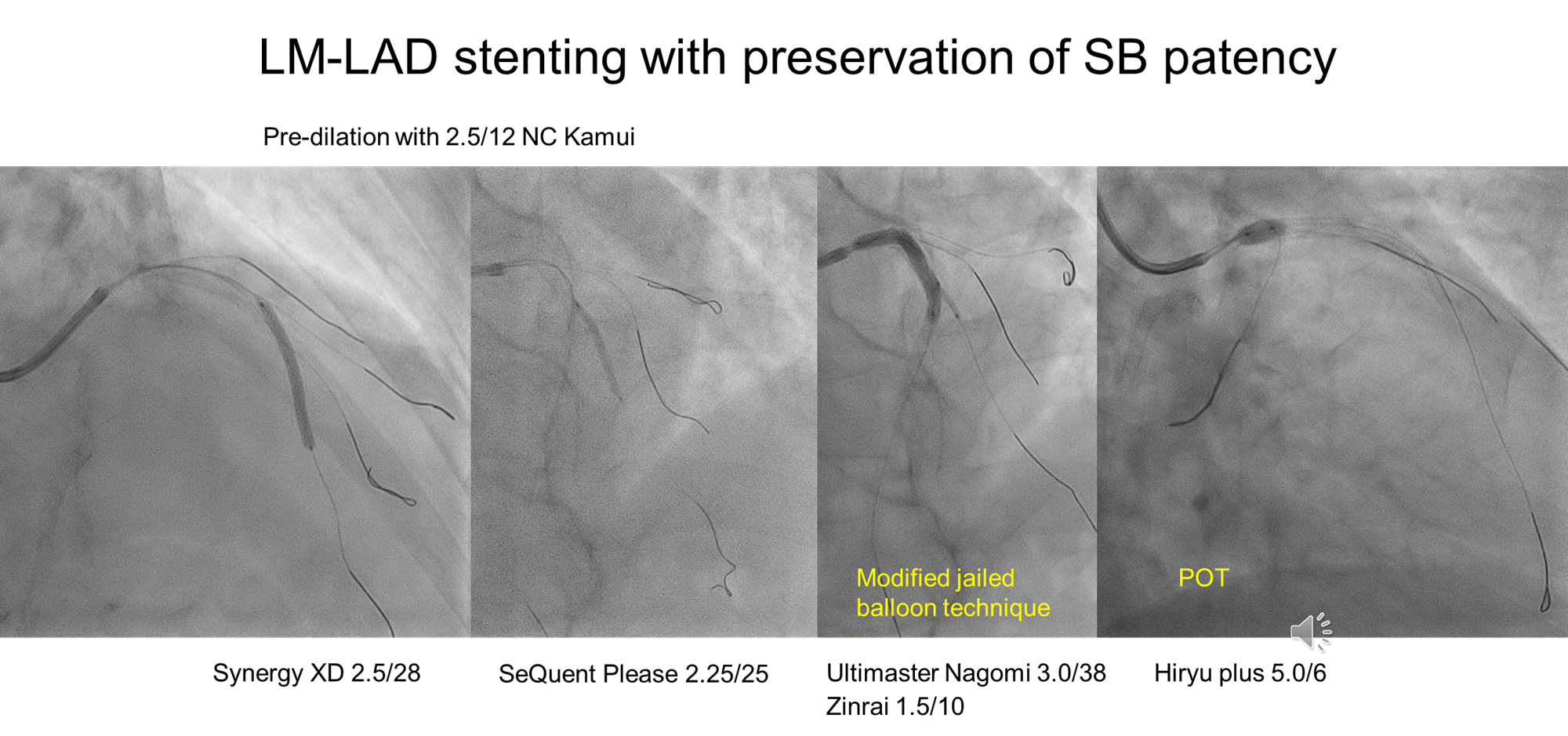
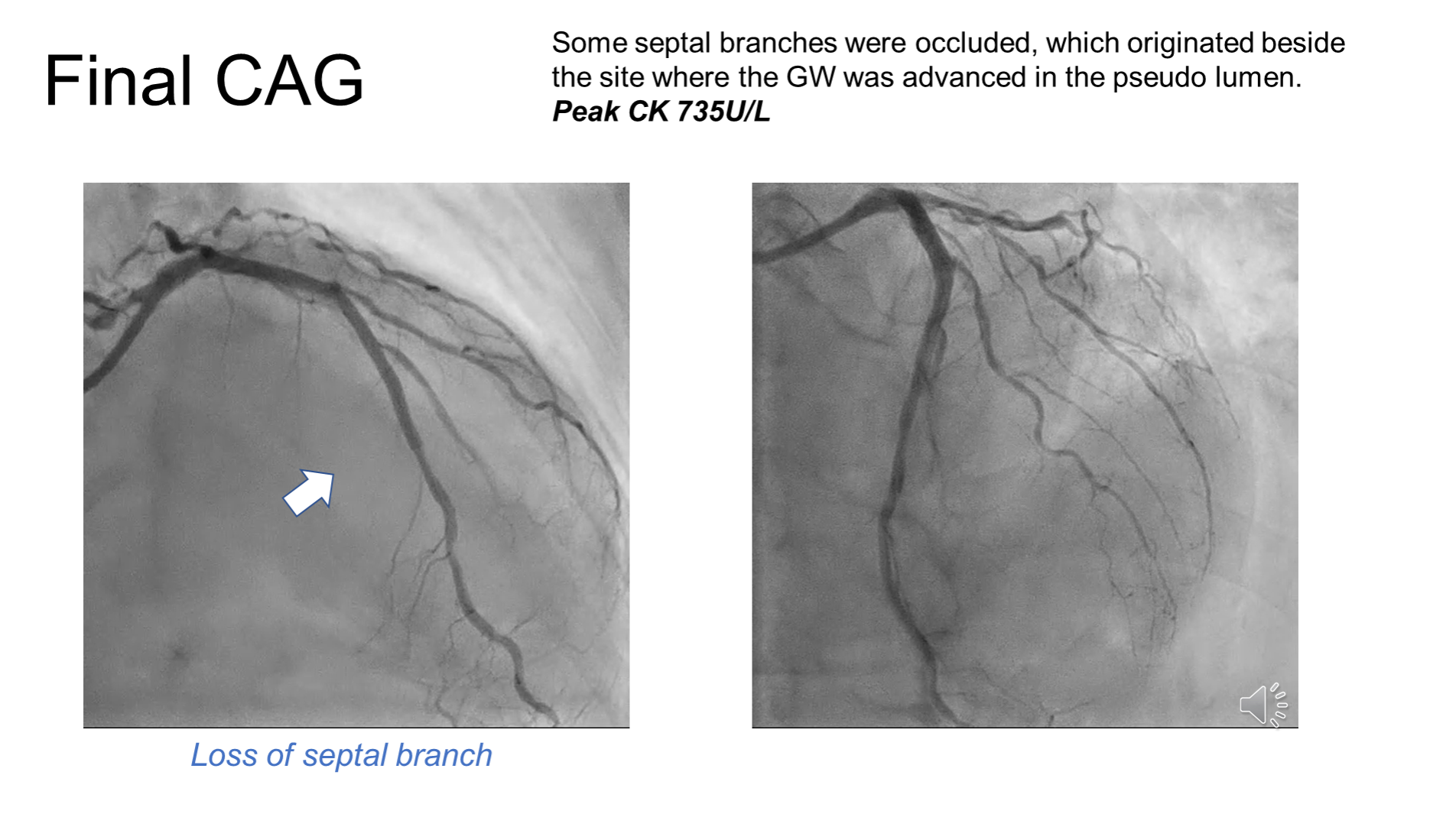
Firstly, guide wire crossed to HL branch and LAD wiring was performed using a double lumen catheter to avoid pseudo lumen wiring. Then, wiring to first and second diagonal branches were achieved. IVUS showed obvious pseudo lumen wiring was limited in the site with 5mm length around second diagonal branch and medial disruption was found in the meddle LAD. Although the eccentric calcified lesion occupied in the half of the vessel, vessel dilation with stenting was thought to be feasible. After predilation with 2.5mm NC balloon, a Synergy 2.5/28mm stent was deployed distally to first diagonal branch in the middle LAD. After pretreatment with a 2.0mm drug-coated balloon in first diagonal branch, a 3.0/38 mm Ultimaser Nagomi stent was deployed from LM ostium to connect the former stent. LM was dilated with a 5.0mm balloon as proximal optimization and LAD was with 3.0mm balloon for sufficient stent expansion with less malapposition. Unfortunately, septal branch close to the site with pseudo lumen wiring in LAD was occluded without jailed wire technique. Finally, minimal stent area in LM, LAD ostium, proximal and middle LAD were widely achieved to 11.1, 8.5, 6.9, and 4.4 mm2, respectively. Although post-procedural CPK was mildly elevated to 735 IU/L, no local left ventricular asynergy was found and chest pain on exertion resolved.
Case Summary
This case presented a complex challenge involving a spiral dissection in the calcified LAD while aiming to preserve multiple side branches during PCI revascularization. The use of IVUS imaging was invaluable for assessing vessel condition, location of guide wire, monitoring the PCI procedure, and guiding safer stent sizing and placement decisions.