
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-068
A Challenging Case Report: Kawasaki Disease With Graft Failure Soon After Coronary Artery Bypass Graft Surgery and Persistent Chest Pain
By Yu Chuan Chuang
Presenter
Yu Chuan Chuang
Authors
Yu Chuan Chuang1
Affiliation
Taichung Veterans General hospital, Taiwan1,
View Study Report
TCTAP C-068
Coronary - Complex PCI - CTO
A Challenging Case Report: Kawasaki Disease With Graft Failure Soon After Coronary Artery Bypass Graft Surgery and Persistent Chest Pain
Yu Chuan Chuang1
Taichung Veterans General hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 41-year-old female suffered non-ST-segment elevation myocardial infarction three months before visiting medical center. The patient underwent coronary artery bypass graft surgery at a local hospital. Nevertheless, she continued to experience discomfort from chest tightness, especially during exertion, with angina classified as Canadian Cardiovascular Society (CCS) class III for three months, despite adhering to optimized medical therapy. An electrocardiogram (ECG) showed sinus rhythm.

Relevant Test Results Prior to Catheterization
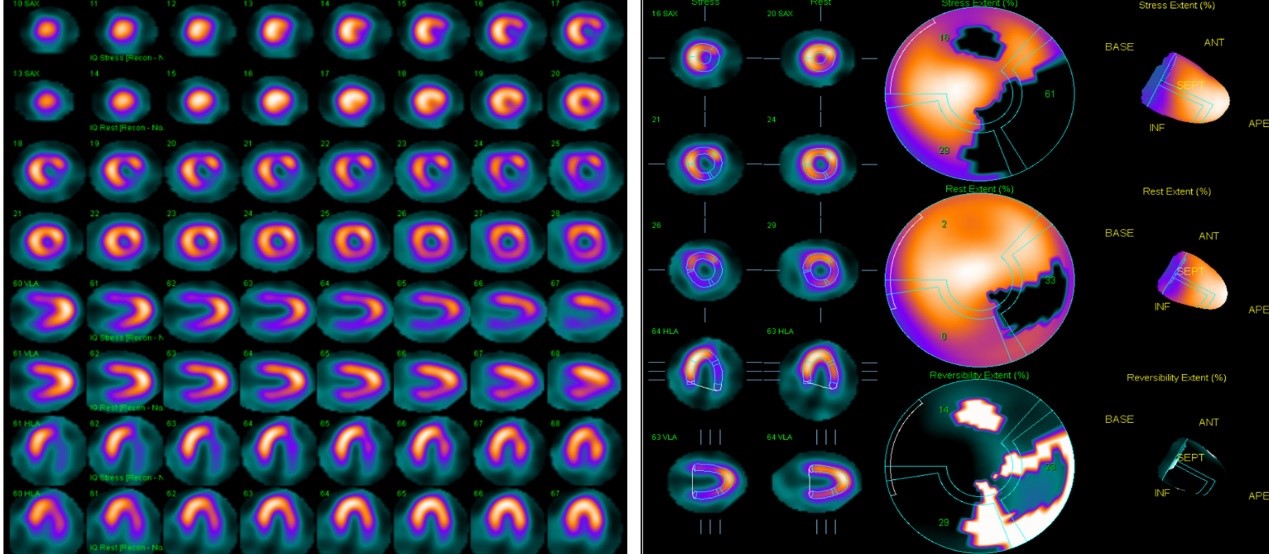
A myocardial perfusion imaging study was conducted, indicating decreasedmyocardial perfusion in the mid to basal anterior wall during pharmacological stresstests using dipyridamole, with significant recovery during rest.Additionally, there was decreased myocardial perfusion in the apical to basallateral wall and the apical to basal inferior wall during pharmacological stresstests, with partial recovery during rest.
Relevant Catheterization Findings
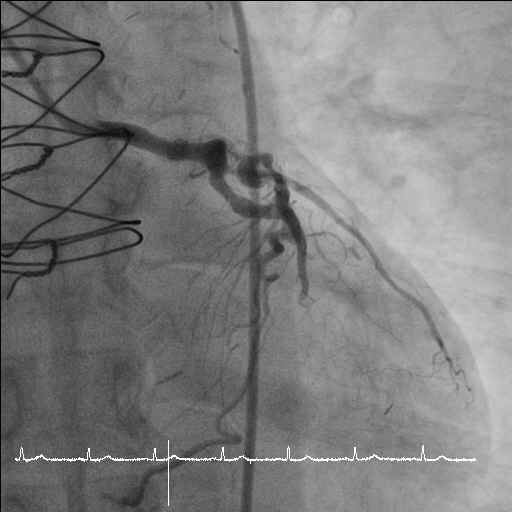
Coronary angiography revealed a 95% discrete eccentric stenosis of the proximal LAD with a well-patent and competitive flow of the left LIMA-LAD-D. A segmental chronic total occlusion of the LCx with a small stump was identified. The saphenous vein graft to the obtuse marginal branch (OM) of the LCx was occluded with stagnant flow in the vessel bed distal to the first obtuse marginal artery (OM-1) occlusion. The RCA was a non-dominant vessel with a very long CTO starting from the RCA ostium.

Interventional Management
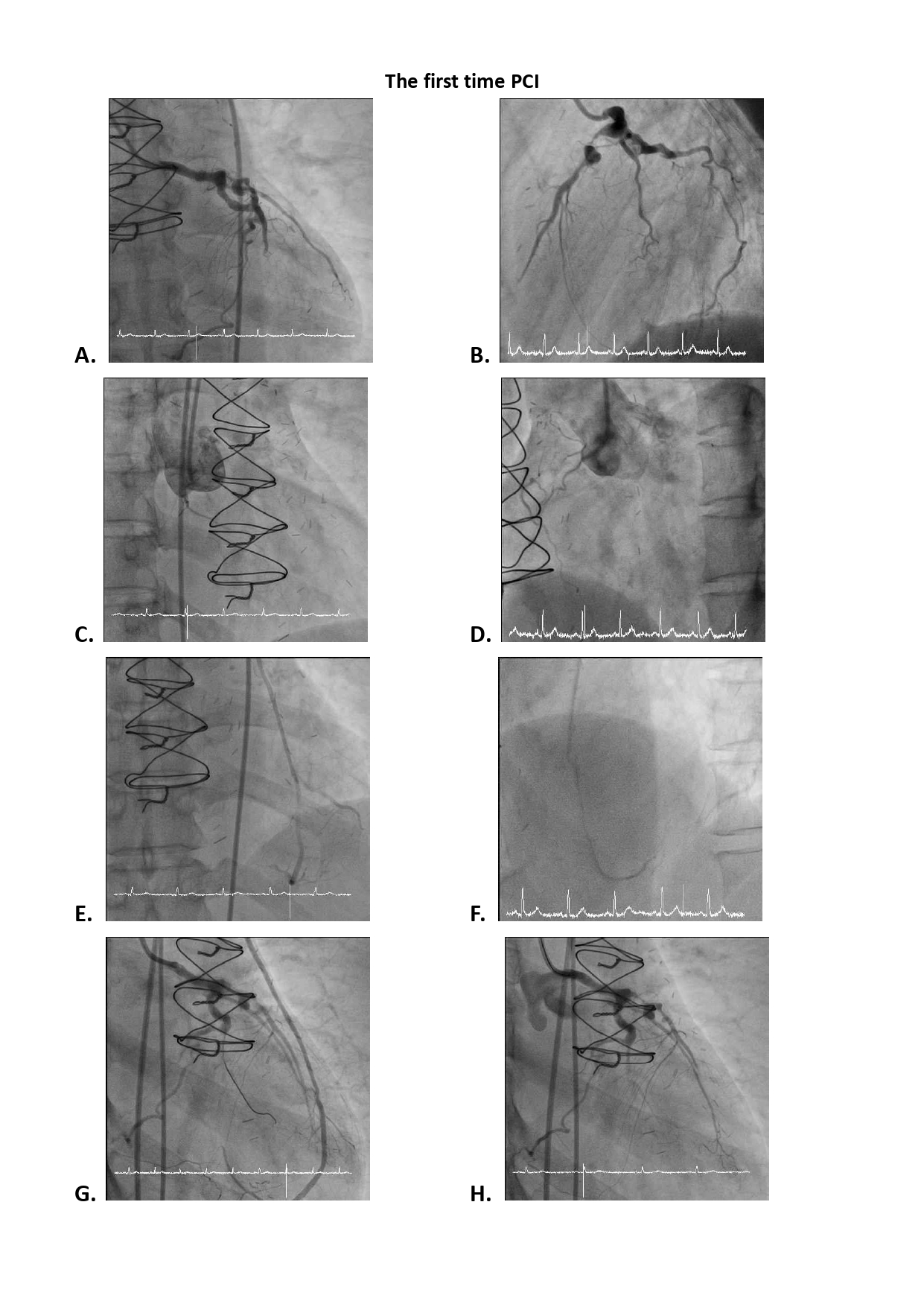
Procedural Step
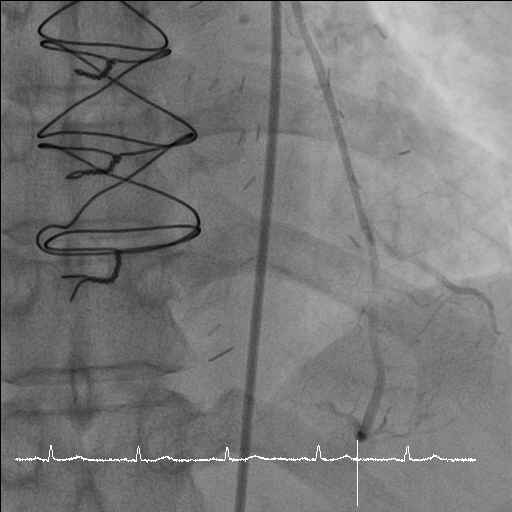
The first PCI focused on the obtuse marginal branch (OM-1) occlusion, and it faced challenges due to the hard, calcified lesions. Multiple dilations with different balloons were attempted, but the main vessel (lower branch) remained inaccessible. The procedure concluded with some progress but not complete revascularization. Two months later, a re-attempt was made, but this time, wiring the OM-1 CTO body proved exceedingly difficult. The minute vessels around the CTO were found to be bridging collaterals rather than the desired microchannel, leading to the abandonment of further attempts.
Three years later, a third PCI was performed due to recurrent angina, revealing severe atherosclerotic changes in the LAD and a long CTO without a stump in the LCx. The RCA was mostly occluded. A PCI procedure was planned to open the LCx via the LAD, but difficulties were encountered when advancing the catheter beyond the stenosis, obstructing blood flow in the native LAD. The procedure shifted focus to treating the stenosis in the LAD to facilitate a retrograde approach in the next session. The LAD was successfully wired and underwent rotational atherectomy, and the final flow in the native LAD was good. A retrograde approach was adopted to tackle the LCx-D CTO. Despite challenging conditions, including heavy calcification, the CTO was eventually crossed using a retrograde approach from LAD, and the LCx was scaffolded with a drug-eluting stent.
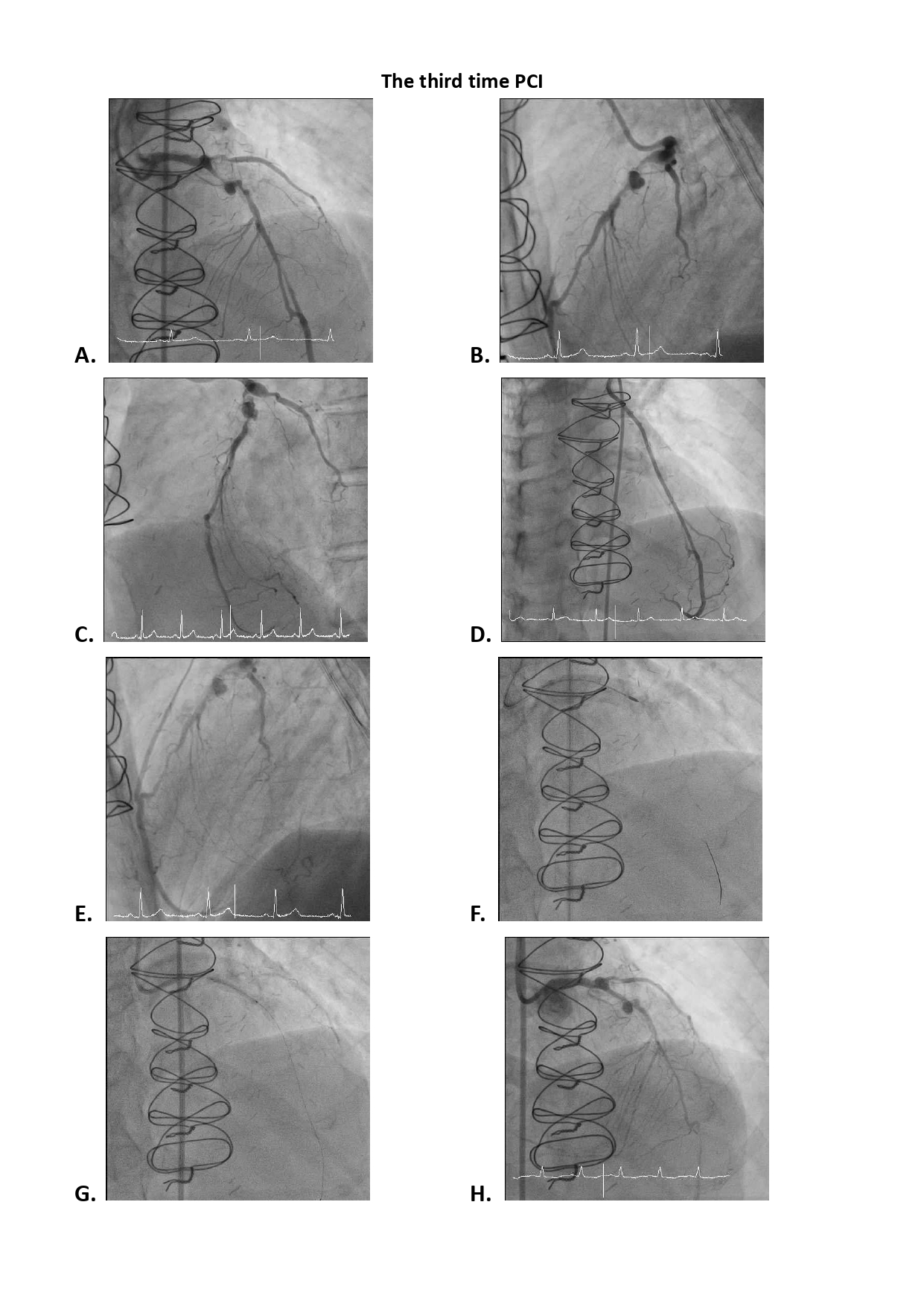
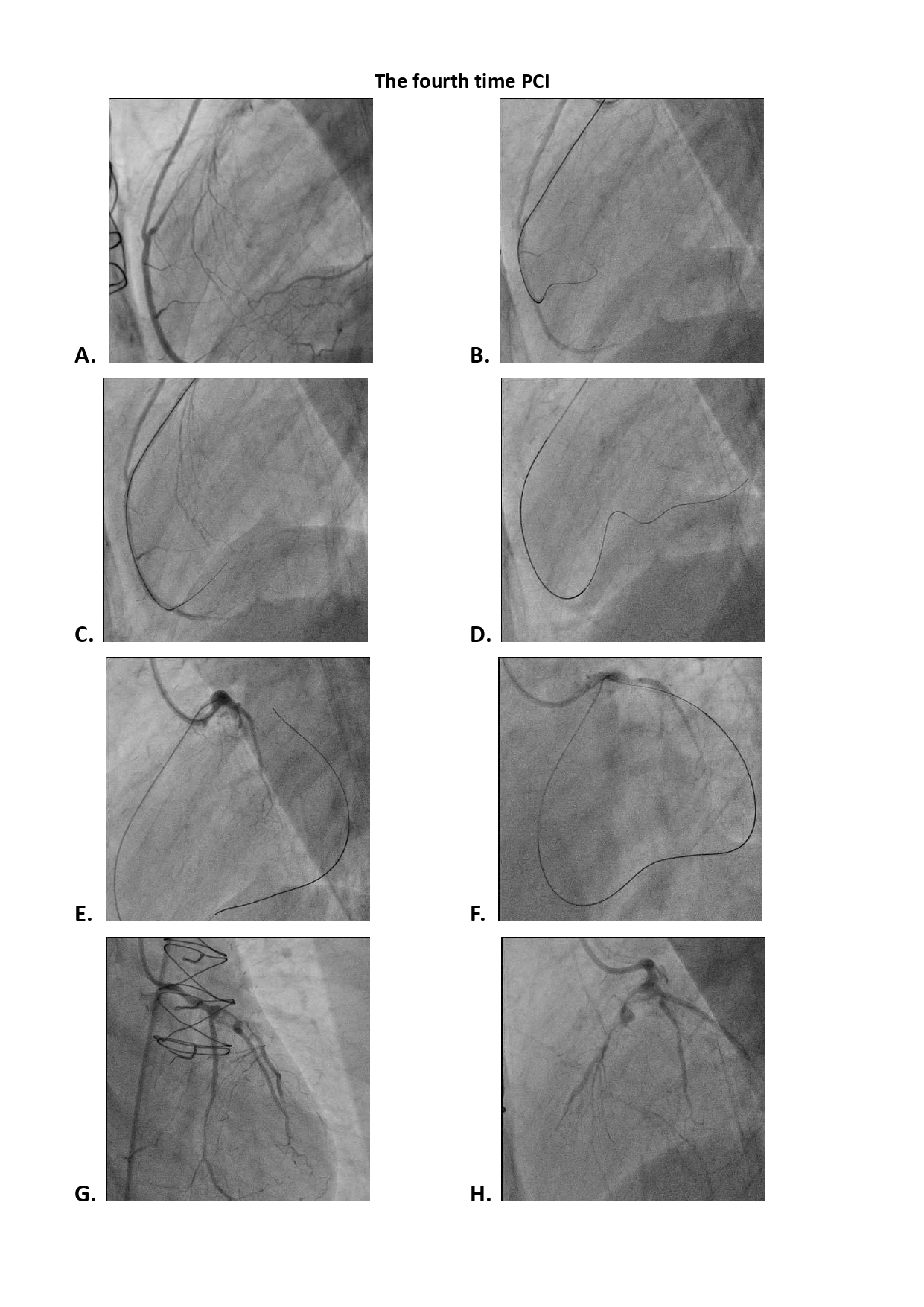
Case Summary
The diagnosis of late cardiovascular sequelae of Kawasaki disease was the most likely etiology for the patient's condition. The patient's complex medical journey, involving multiple attempts to address chronic total occlusions and stenoses in her coronary arteries, as well as the need for innovative and flexible approaches in the face of challenging lesions and complications. The PCI procedure was performed to open the LCx via the LAD, the CTO was eventually crossed using a retrograde approach, and the LCx was scaffolded with a drug-eluting stent. Late cardiovascular sequelae of Kawasaki disease underscores the importance of considering less common etiologies in such cases.