
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-014
ST-Segment Depression in AVL: A Strong Predictor of Inferior Occlusion Myocardial Infarction (OMI)
By Ahmad Faisal Badaruddin, Khai Chih Teh
Presenter
AHMAD FAISAL BADARUDDIN
Authors
Ahmad Faisal Badaruddin1, Khai Chih Teh1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-014
Coronary - ACS/AMI
ST-Segment Depression in AVL: A Strong Predictor of Inferior Occlusion Myocardial Infarction (OMI)
Ahmad Faisal Badaruddin1, Khai Chih Teh1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
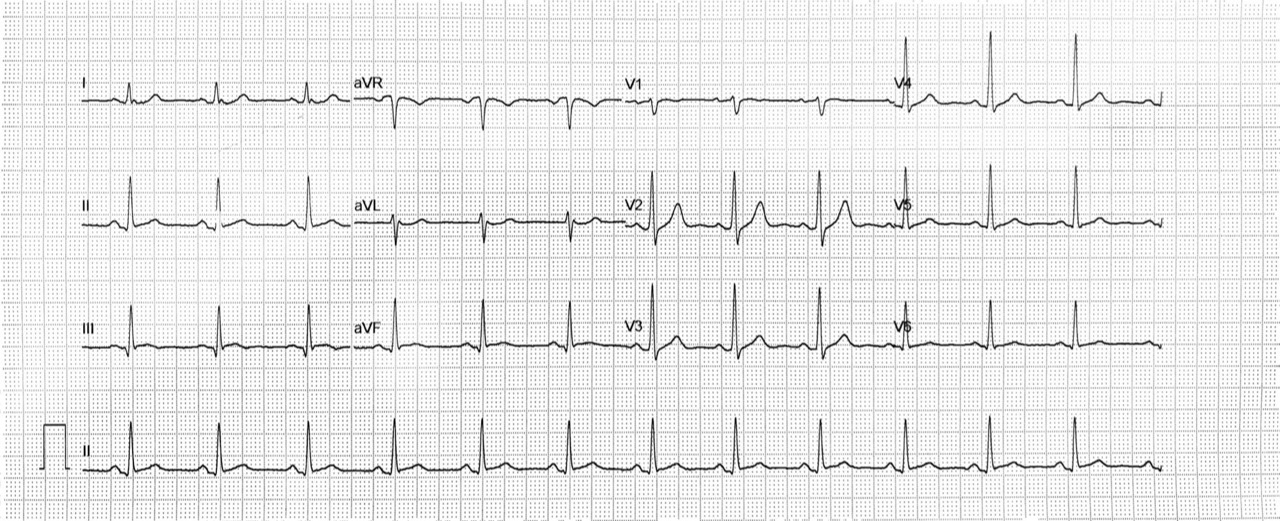
A 60-year-old gentleman with a known case of DM and hypertension defaulted treatment. He presented to an emergency department in a private hospital with chest pain less than 9 hours after onset, heaviness, non-radiating and pain score reduced from 9 to 2. Blood pressure was 120/92 mmHg, with a heart rate of 121 bpm. An electrocardiogram (ECG) showed sinus rhythm with no acute evolving changes. He was transferred to our hospital for further cardiac assessment.
Relevant Test Results Prior to Catheterization
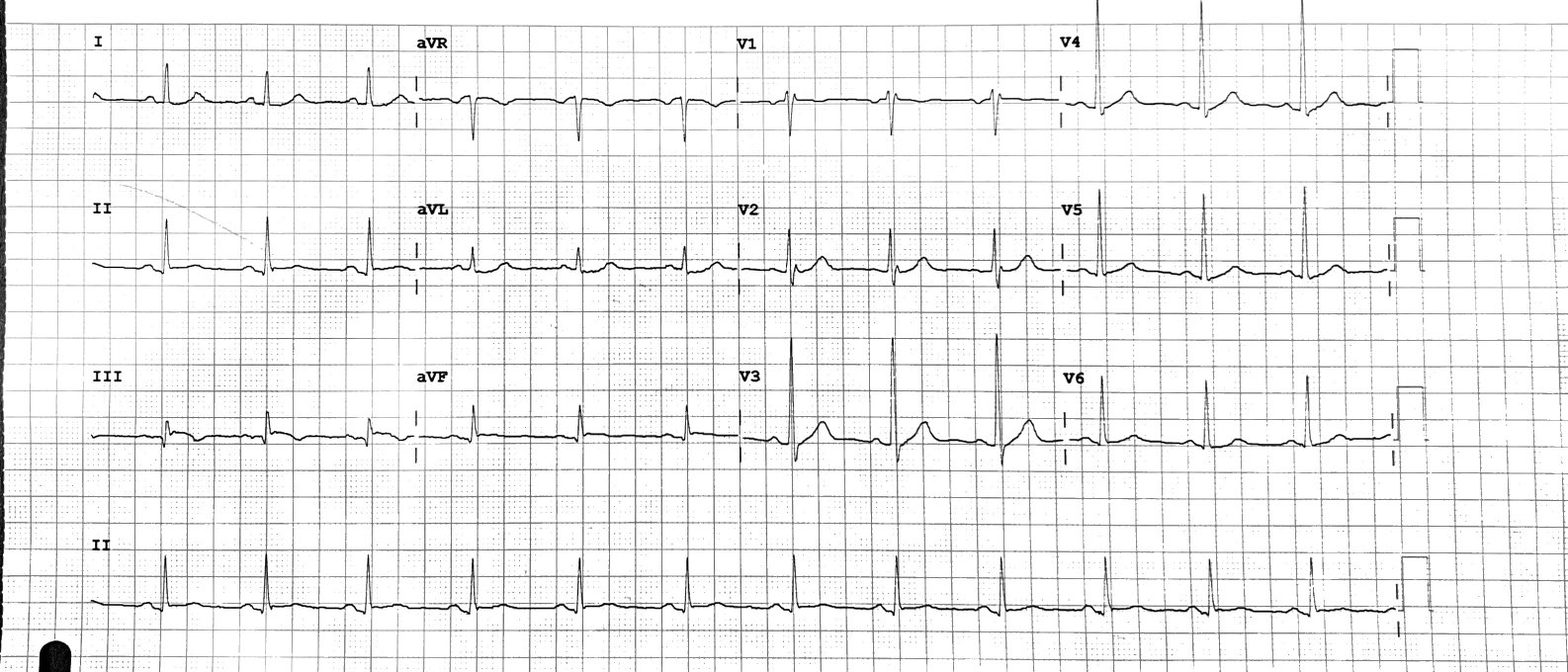
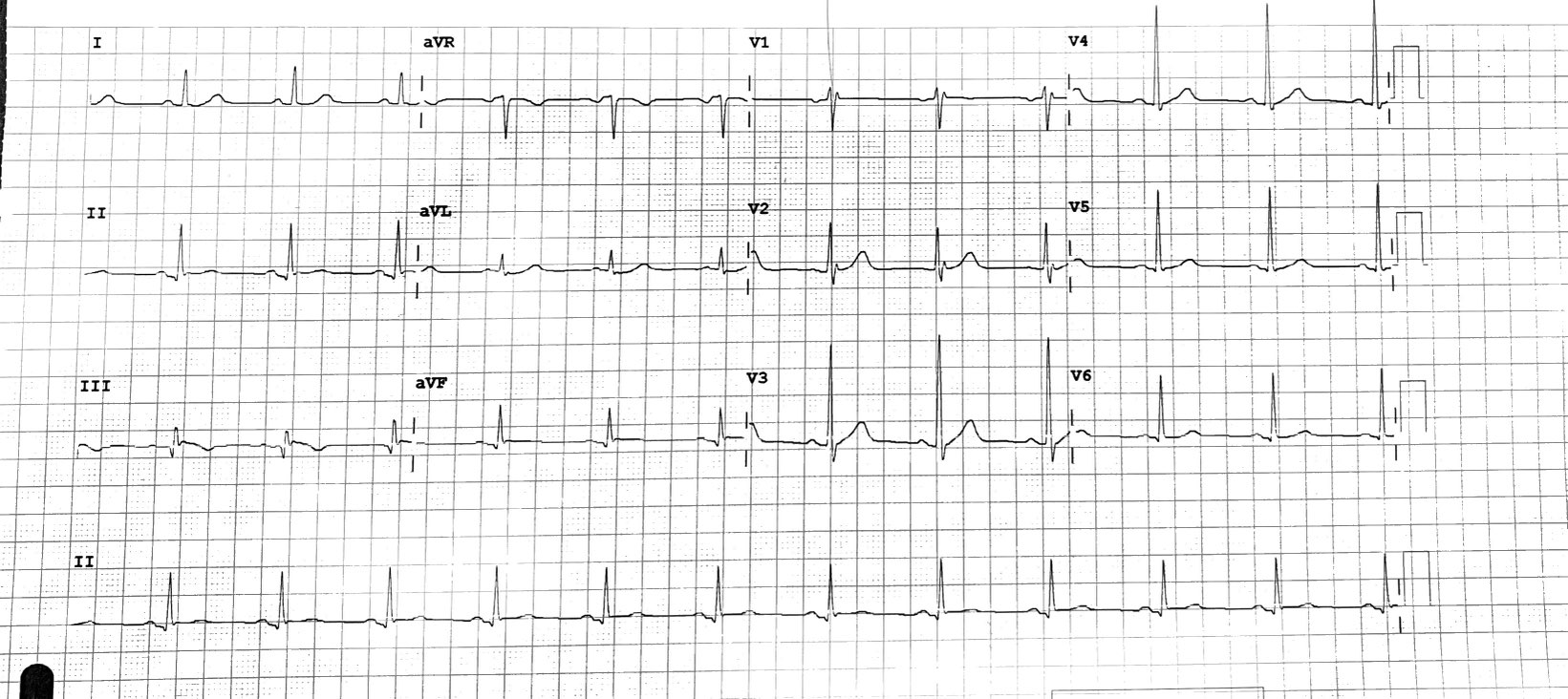
When the patient arrived at our Emergency Department, he reported feeling minimal chest discomfort. His blood pressure was 127/63 mmHg, and his heart rate was 74 bpm. An ECG was performed, which showed ST-segment elevation in lead II, along with reciprocal ST-segment depression in AVL. The patient's cardiac markers were also measured, with Troponin T at 502 pg/ml, Creatinine Kinase (CK) at 931 U/l, and CKMB at 100 U/l. The diagnosis was acute inferior ST-elevation myocardial infarction (STEMI).
Relevant Catheterization Findings
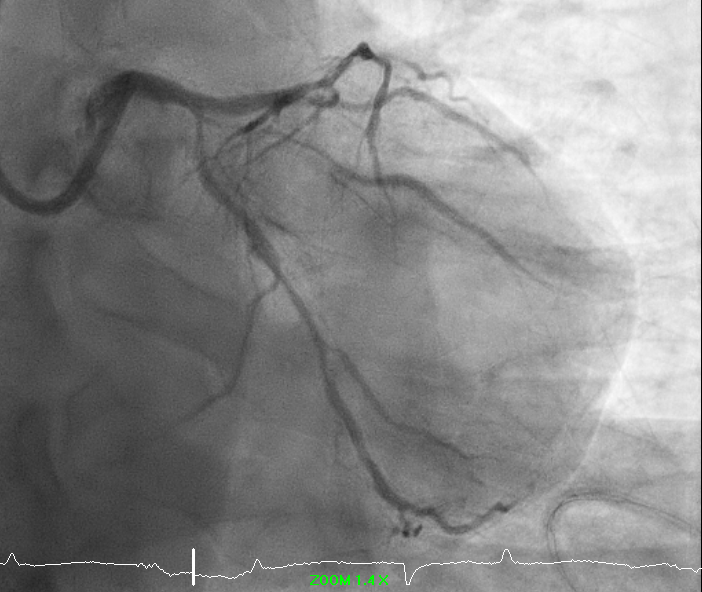
Primary percutaneous coronary intervention (PCI) was activated. The vessel was assessed using right radial approach. The left system was engaged using EBU 3.5 6 Fr, which showed mild disease distal left main stem, mild disease proximal to diagonal with long diffuse until distal left anterior descending artery (LAD), and severe ostial disease left circumflex artery (LCX) with moderate diffuse lesion. The right system showed total occlusion middle segment of the right coronary artery (RCA).
Interventional Management
Procedural Step
A guiding catheter JR 3.5 6Fr was used to engage the right system. Runthrough floppy was used to wire down to the posterolateral (PL) branch. Thromboaspiration using Thrombuster was performed, which revealed a red thrombus, but it was unable to pass the mid-segment RCA due to severe stenosis. Percutaneous Old Balloon Angioplasty (POBA) with a semi-compliant balloon 2.0/15mm was used, and Timi III flow was established with no dissection. Given triple vessel disease (TVD) as the diagnosis, we decided to stop the procedure and consider a coronary artery bypass graft (CABG) as the best option for revascularization.


Case Summary
A case of occlusion myocardial infarction (OMI) is presented in this report. The patient complained of angina, but the ECG changes did not indicate the extent of myocardial infarction (MI) severity. However, the presence of ST segment depression in AVL raised concerns of significant MI. As per the angiogram report, he was found to have OMI in the right coronary artery, along with diffuse disease of other coronaries. Studies have shown that ST segment depression in AVL is more commonly associated with infarcts in the right coronary artery. This case highlights the significance of reciprocal changes of ST segment depression in AVL as an early predictor of Inferior MI.