
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-063
Guide Extension Facilitate Externalization in Retrograde CTO PCI
By Bogie Putra Palinggi, Doni Firman, Amir Aziz Alkatiri, Arwin Saleh Mangkuanom, Nanda Iryuza
Presenter
Bogie Putra Palinggi
Authors
Bogie Putra Palinggi1, Doni Firman1, Amir Aziz Alkatiri1, Arwin Saleh Mangkuanom1, Nanda Iryuza1
Affiliation
National Cardiovascular Center Harapan Kita, Indonesia1,
View Study Report
TCTAP C-063
Coronary - Complex PCI - CTO
Guide Extension Facilitate Externalization in Retrograde CTO PCI
Bogie Putra Palinggi1, Doni Firman1, Amir Aziz Alkatiri1, Arwin Saleh Mangkuanom1, Nanda Iryuza1
National Cardiovascular Center Harapan Kita, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Relevant Test Results Prior to Catheterization

Relevant Catheterization Findings

Interventional Management
Procedural Step
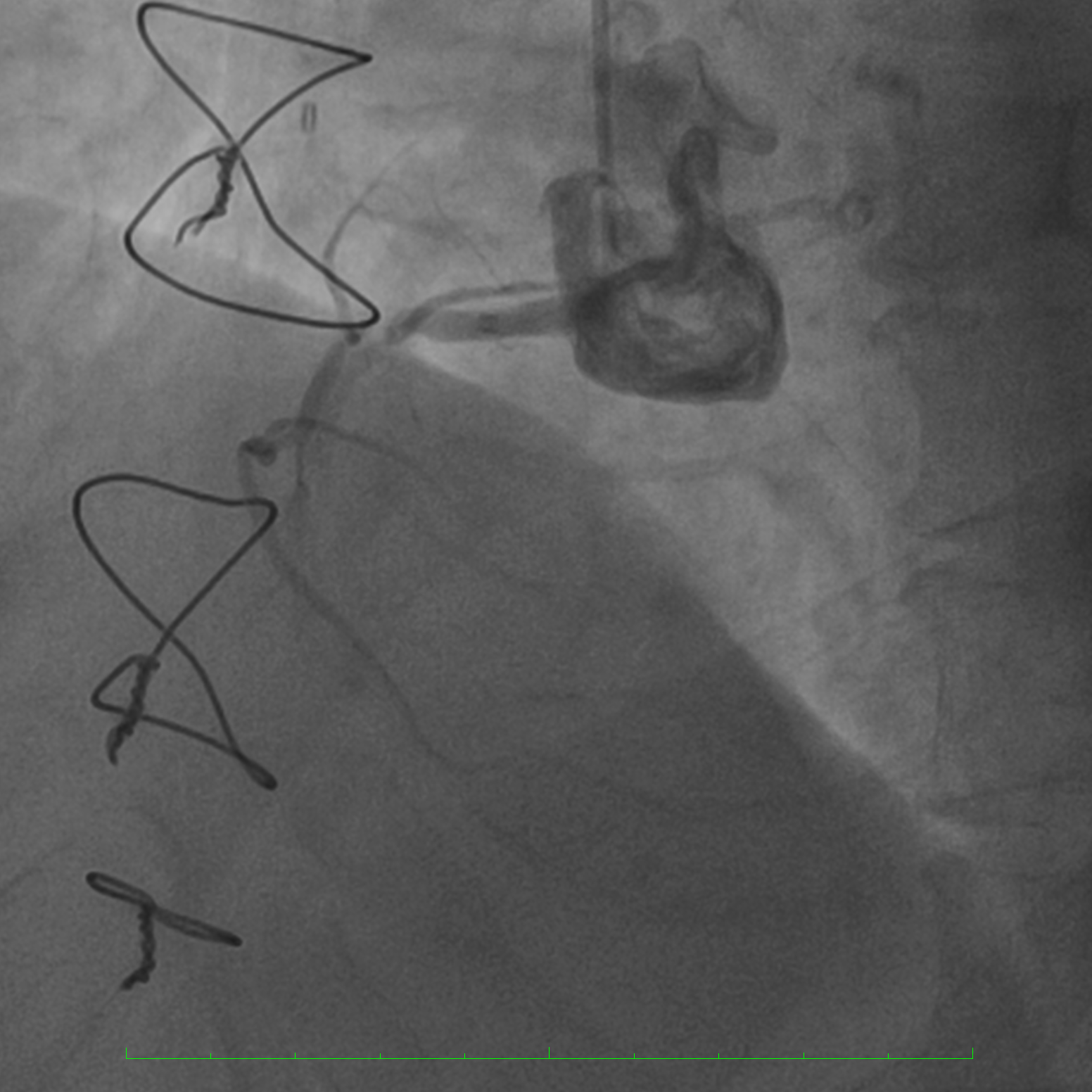
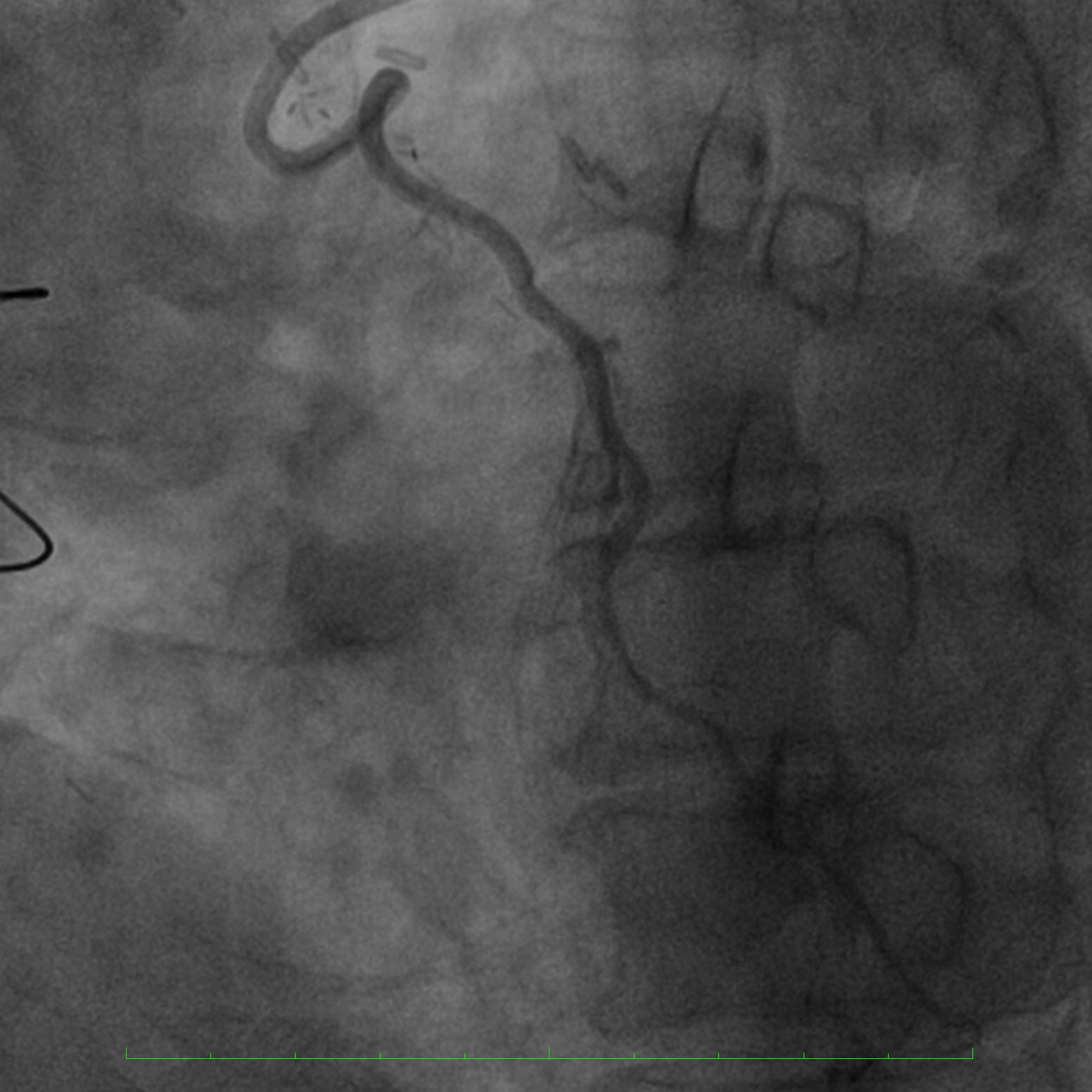
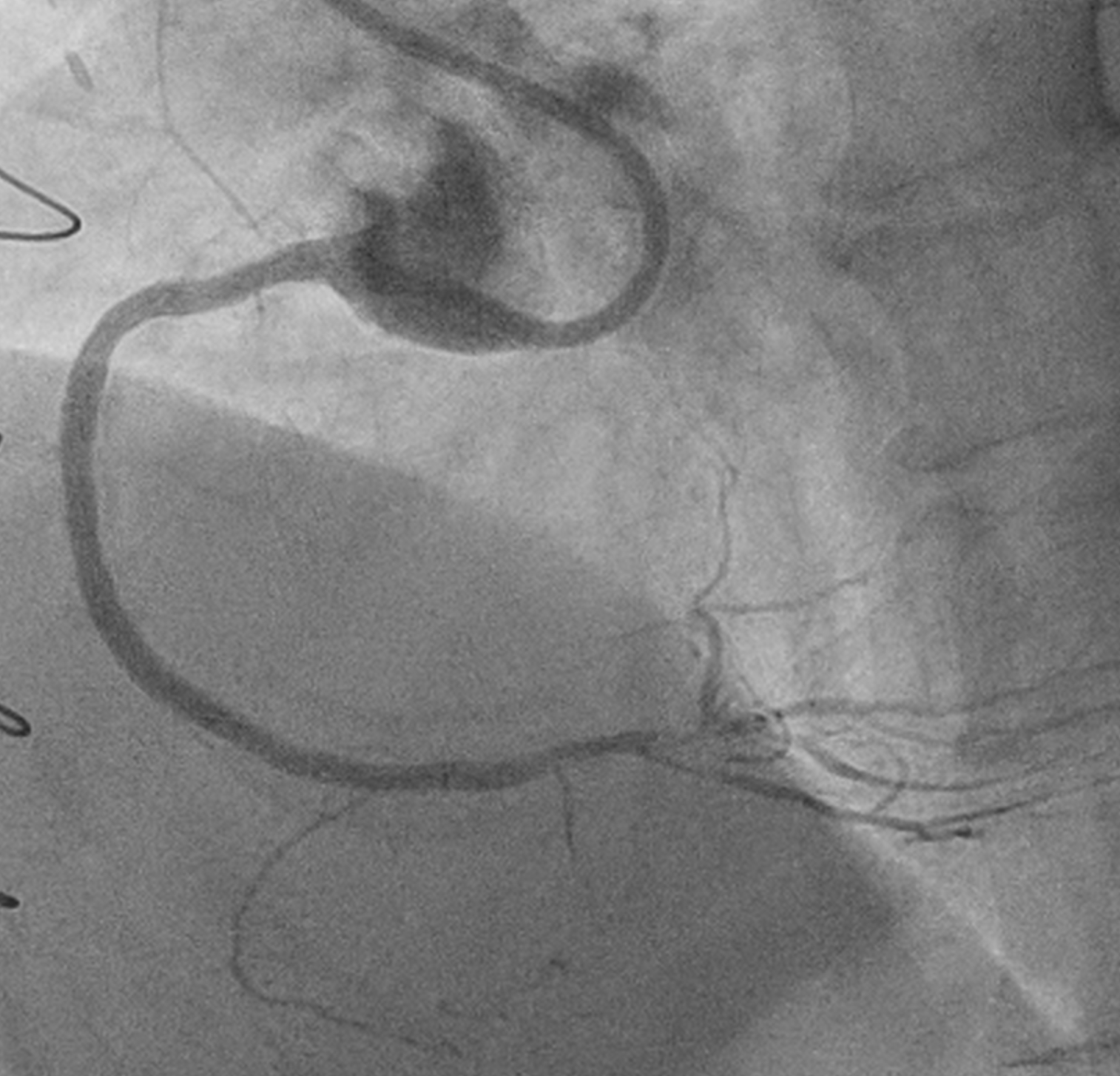
Right femoral 45 cm long sheath 7 Fr and right radial 6 Fr conventional sheath was used for vascular access. AL 0.75 side hole 7 Fr and XB 3.5 6 Fr guiding catheters through right femoral and right radial access were used to engage Right Coronary Artery and Left Coronary Artery, respectively. An antegrade approach with guidance of retrograde wire was chosen as strategy. Therefore, after identifying a septal collateral emerging from the proximal Left Anterior Descending, collateral navigation with Suoh 03 backed up Corsair Pro XS 155 cm Microcahteter (MC) was successfully performed. Further antegrade attempt using Miracle 3 and Gladius EX 14 wire with Corsair Pro 135 cm MC was unsuccessful. Subsequently, a retrograde approach with reverse controlled antegrade and retrograde subintimal tracking (CART) was chosen as secondary strategy. Attempt of connecting antegrade and retrograde channel with balloon inflation (1,5 mm and 2.0 mm semi compliant (SC) balloons) over the antegrade wire was performed but failed. A guide catheter extension (Guideliner 6F) is advanced over the antegrade guidewire followed by balloon dilatation (2.5 mm and 3.0 mm SC balloons). After predilatation with balloons, we were able to advance the Retrograde (RG 3) wire and MC beyond the distal cap of the occlusion into the guidecatheter extension. Retrograde wire was externalized and used for subsequent angioplasty with 3.0 mm Non Compliant balloon. Drug Eluting Stents 2.5/30 mm and 3.0/38 mm was implanted with an excellent result.


Case Summary
The reverse controlled antegrade and retrograde subintimal tracking (CART) is the most commonly used technique for retrograde chronic total occlusion percutaneous coronary intervention. Guide extension can be particularly useful if reverse CART is challenging to complete.