
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-183
Spontaneous Recanalization of Coronary Thrombus in a SLE Case Presenting as Acute Myocardial Infarction
By Yiting Wu, Feng Yu Kuo
Presenter
Yiting Wu
Authors
Yiting Wu1, Feng Yu Kuo1
Affiliation
Kaohsiung Veterans General Hospital, Taiwan1,
View Study Report
TCTAP C-183
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
Spontaneous Recanalization of Coronary Thrombus in a SLE Case Presenting as Acute Myocardial Infarction
Yiting Wu1, Feng Yu Kuo1
Kaohsiung Veterans General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
This 48-year-old female had history of systemic lupus erythematosus, pulmonary embolism. She suddenly collapsed at home 30 minutes before sent to ER. EMT arrived and AED defibrillation twice were performed. Upon arrival to ER, GCS E1V1M1 and no palpable pulse, OHCA noted. CPR was performed, then after 5 minutes ROSC.Physical examination found some erythematous psoriasis form rash over her dorsal hand, and trivial systolic murmur. The remainder of the examination was normal.

Relevant Test Results Prior to Catheterization
Laboratory test revealed leukocytosis, significant hyperlactatemia, abnormal cardiac biomarkers.
Electrocardiogram showed ST elevation over anterior leads V1-V5 with inferior lead reciprocal change, suspect anterior STEMI. Primary PCI was arranged.Echocardiogram revealed mildly reduced LVEF(EF43%), mild concentric left ventricle hypertrophy.
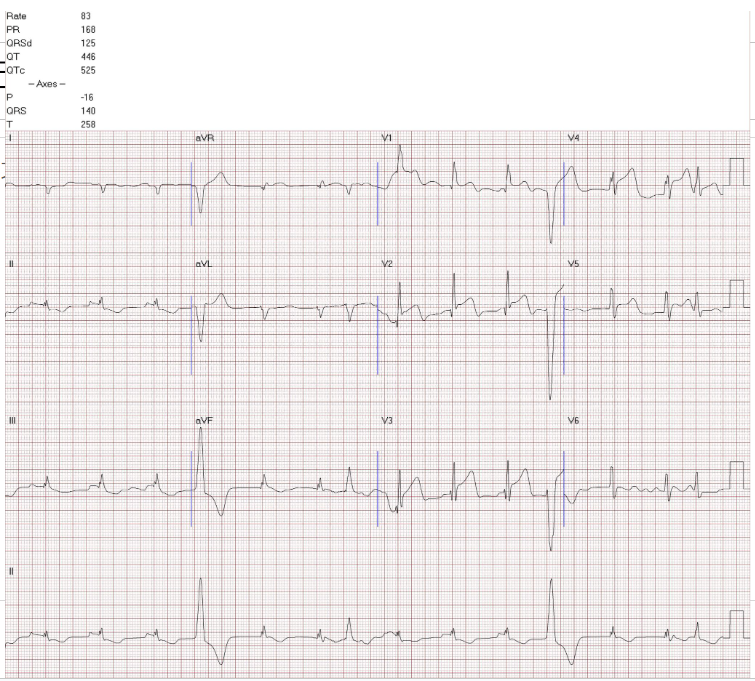
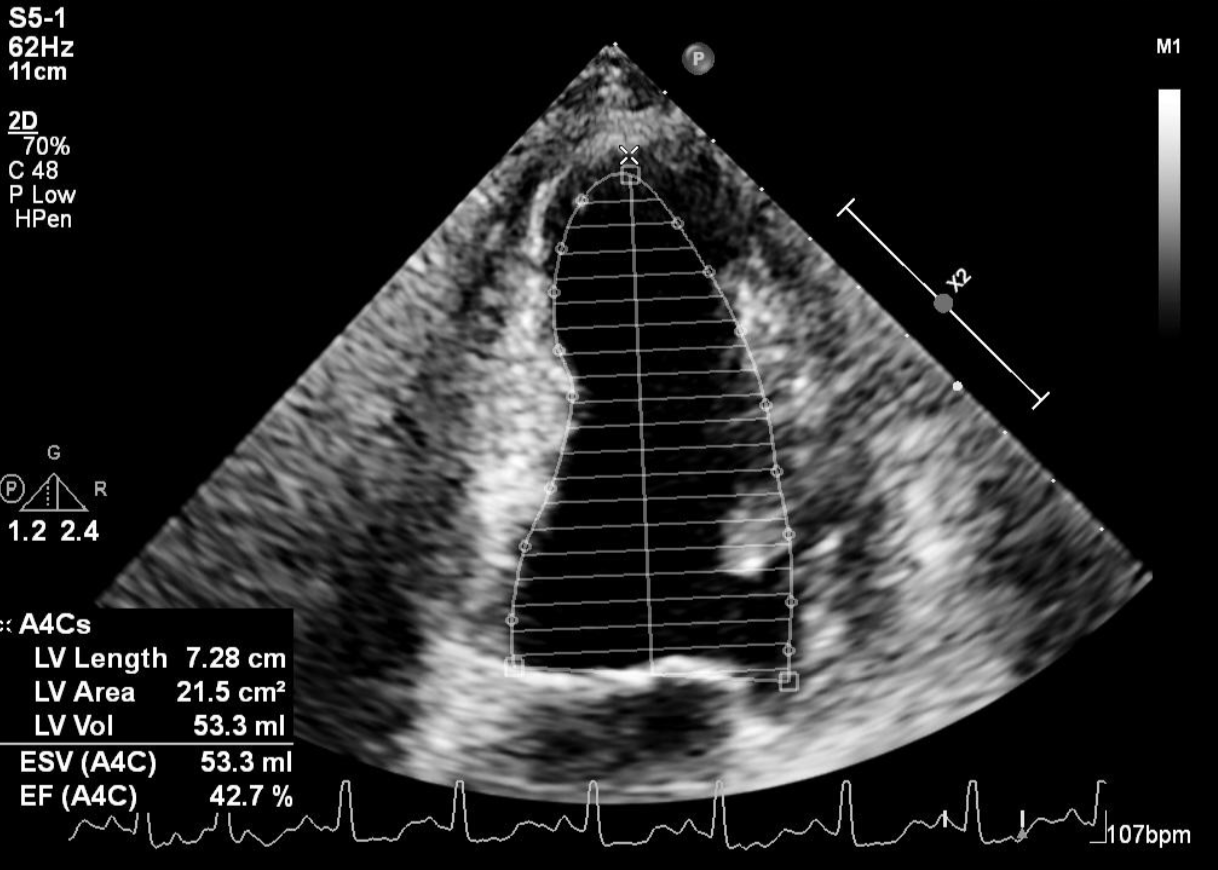
Electrocardiogram showed ST elevation over anterior leads V1-V5 with inferior lead reciprocal change, suspect anterior STEMI. Primary PCI was arranged.Echocardiogram revealed mildly reduced LVEF(EF43%), mild concentric left ventricle hypertrophy.
Relevant Catheterization Findings
Coronary angiogram showed left anterior descending artery middle segment 70% stenosis with hazziness and suspect dissection flap. The blood flow of the LAD was grade II according to TIMI scoring system. Right coronary artery, left circumflex artery showed no significant stenosis.

Interventional Management
Procedural Step
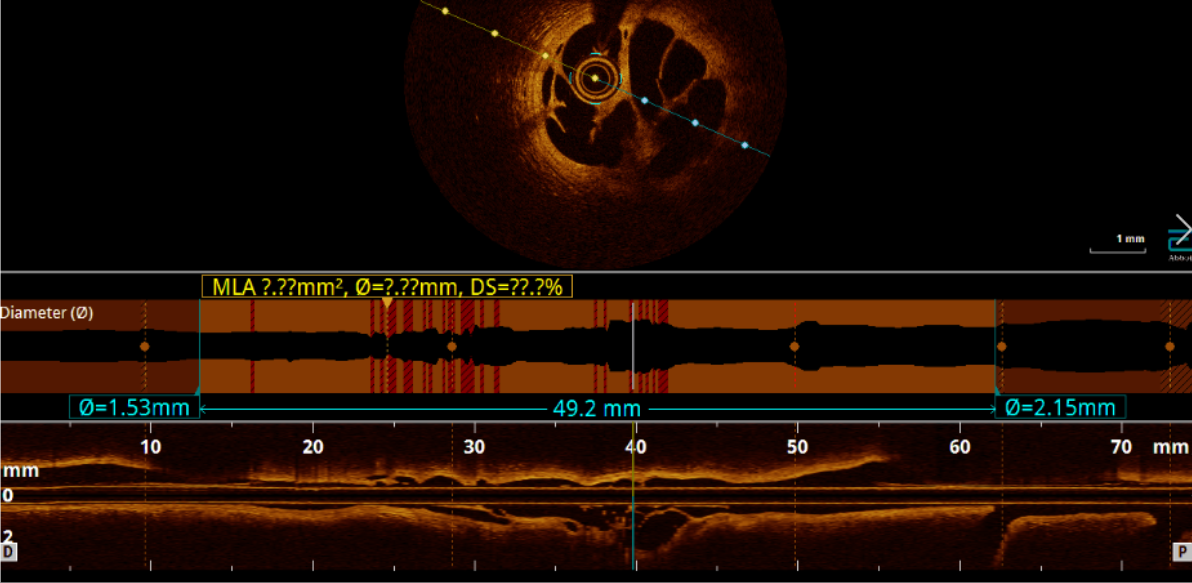
We approached the lesion using Runthrough wire through left anterior artery (LAD) smoothly. We decided to evaluate the lesion by optical coherence tomography (OCT).Cross-sectional OCT images acquired from the LAD-P to -M lesion revealed a honeycomb-like structure. The proximal lesion showed intima tissue mixed with fibrous tissue (high signal intensity, low signal attenuation) and atheroma (low signal intensity, high signal attenuation). The LAD-M lesion was dilated by a 2.5mmx20mm balloon. We approached by Sion blue wire to LAD-Diagonal 2 branch. The LAD-Diagonal 2 branch lesion was dilated by 2.0x15mm balloon. A 2.5x48mm stent was deployed for LAD-M to-D. A 3.0x20 mm stent was deployed for LAD-M. Post dilatation was done. Both OCT and angiogram demonstrated a good final result with TIMI 3 flow.


Case Summary
The underlying mechanisms of spontaneous recanalized coronary thrombus include in situ thrombus, cardiac embolism, dissection of an atherosclerotic plaque, and post-spontaneous dissection. The patient had SLE disease which is associated with spontaneous coronary dissection. However, OCT revealed the atheroma at the proximal LAD. Therefore, the SRCT lesion is more likely related to the mechanism of dissection of an atherosclerotic plaque. SLE has a significant correlation with coronary atherosclerosis. Notably, this is the first reported case of SRCT in a patient with SLE, which may related to the potential mechanisms for such lesions.