
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-057
Retrieving Stuck RG3 in the Severely Calcified Chronic Total Occlusion of RCA
By Haw-Ting Tai, Kenya Nasu, Po-Ming Ku, Feng Yu Kuo
Presenter
Haw-Ting Tai
Authors
Haw-Ting Tai1, Kenya Nasu2, Po-Ming Ku3, Feng Yu Kuo1
Affiliation
Kaohsiung Veterans General Hospital, Taiwan1, Mie Heart Center, Japan2, Chi Mei Medical Center, Taiwan3,
View Study Report
TCTAP C-057
Coronary - Complex PCI - CTO
Retrieving Stuck RG3 in the Severely Calcified Chronic Total Occlusion of RCA
Haw-Ting Tai1, Kenya Nasu2, Po-Ming Ku3, Feng Yu Kuo1
Kaohsiung Veterans General Hospital, Taiwan1, Mie Heart Center, Japan2, Chi Mei Medical Center, Taiwan3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
The 78-year-old woman had end-stage renal disease undergoing regular hemodialysis (HD), hypertension, dyslipidemia, and persistent atrial fibrillation. She had intermittent chest pain and had been hospitalized for non-ST-elevation myocardial infarction, following unsuccessful percutaneous coronary intervention (PCI), and congestive heart failure. The physical examination showed clear breathing sounds, irregular heartbeats with soft systolic murmurs, and no pitting edema in extremities.

Relevant Test Results Prior to Catheterization
Transthoracic echocardiography showed a left ventricular ejection fraction of 50% with hypokinesia in the basal inferoposterior wall, and moderate mitral regurgitation. Myocardial perfusion scan detected possible myocardial ischemia in the apex and anteroseptal wall. Computerized tomography coronary angiogram (CCTA) showed calcified lesions in the left anterior descending artery (LAD), left circumflex artery (LCx) and right coronary artery (RCA) including severe calcification at the ostial RCA.
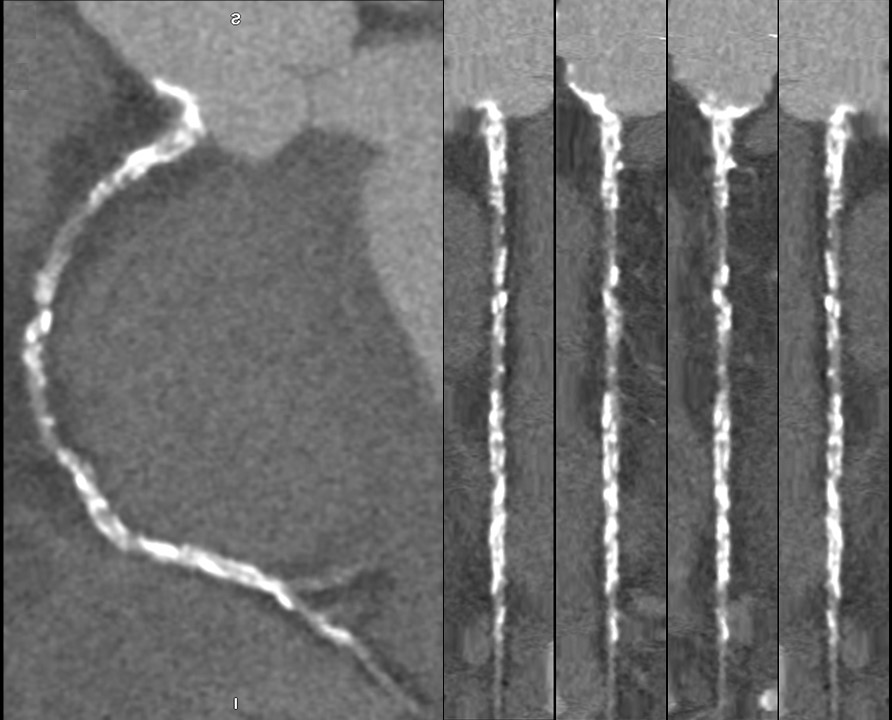
Relevant Catheterization Findings
Coronary angiography revealed a chronic total occlusion (CTO) at the RCA ostium with heavy calcification, diffuse disease in the proximal to middle segment of the LAD with an 80% stenosis, and focal 70% stenosis in the distal LCx and obtuse marginal branch. Abundant collateral flow from the distal LCx and septal branches of the LAD towards the RCA was noted, farthest reaching the proximal RCA.


Interventional Management
Procedural Step
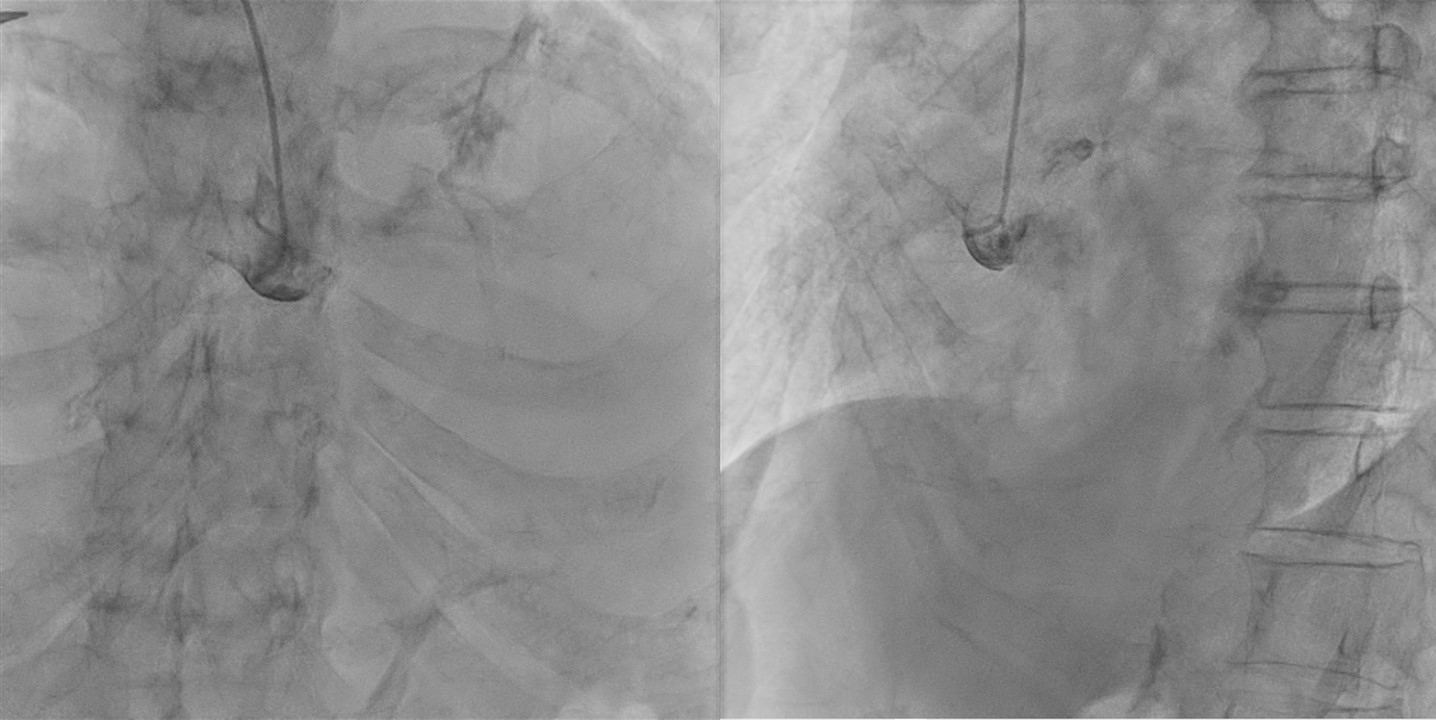
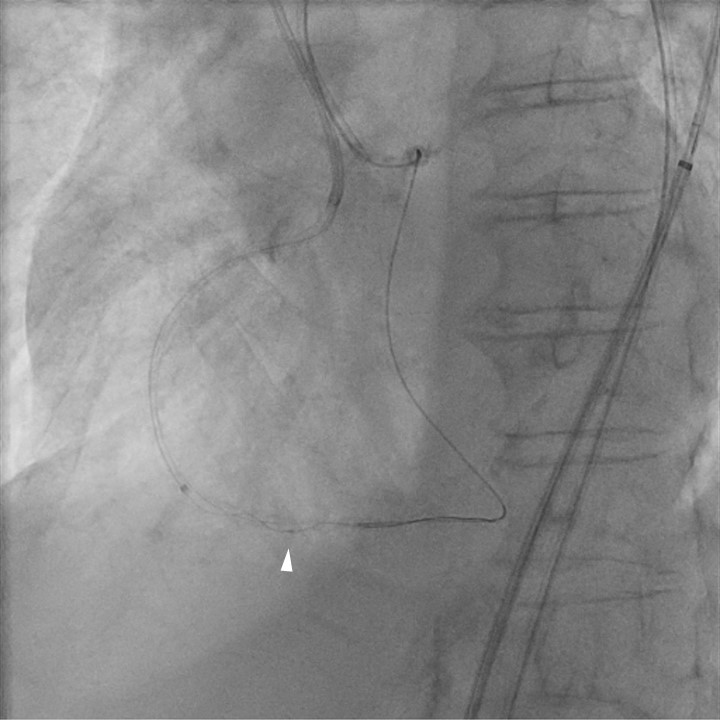
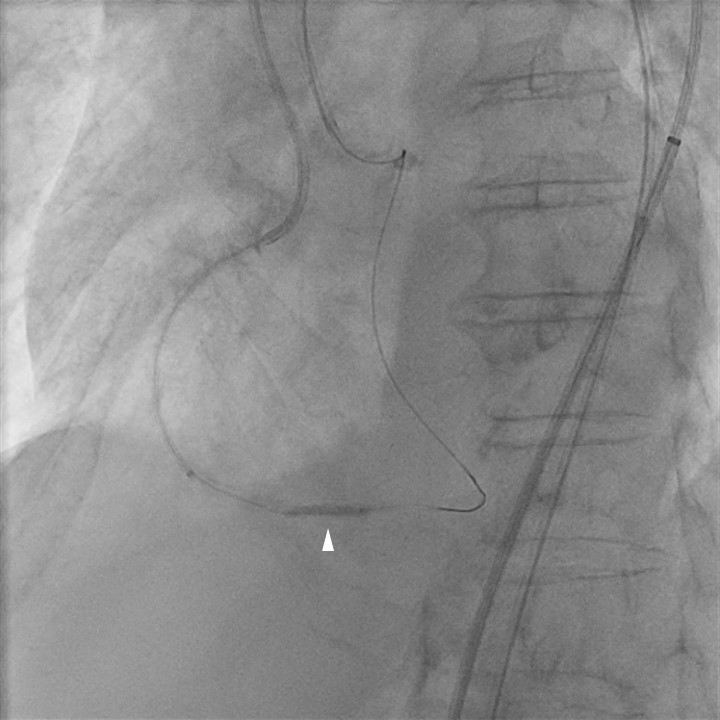
The PCI began with left coronary artery engagement using an extra backup catheter via femoral access. A guidewire and a microcatheter (MC) were advanced to the proximal RCA just before the CTO, retrogradely through a septal branch of LAD. After unsuccessful attempts to cross the CTO, including retrograde and then antegrade punctures with CTO wires via a short Amplatz left catheter, the electrocaumetry-facilitated crossing (ECFC) (50 Watts for 4 times) allowed the retrograde wire to penetrate the CTO. As the retrograde MC could not pass through the severely calcified lesion, the retrograde wire was changed to a RG3 wire (Asahi Intecc), which is captured and externalized with the use of snare, and antegrade percutaneous transluminal coronary angioplasty (PTCA) and stenting over ostial to proximal RCA were done smoothly. However, the RG3 wire could not be retrieved, seemingly trapped within the calcified lesion over distal RCA with difficulty in passing balloons. After antegrade wiring through the stuck site with balloons inflation, we still failed passing a 1.0 mm balloon via the RG3 wire with the support of an extension catheter. A retrograde Tornus 88Flex MC (Asahi Intecc) passed and then allowed an antegrade 2.25 mm balloon inflated to 24 atms at the stuck site. Retrieving the RG3 wire finally succeeded after advancing retrograde Corsair Pro XS MC (Asahi Intecc) into the antegrade extension catheter. The final angiogram showed no complication.

Case Summary
We presented a case of CTO at RCA with device entrapment, including the use of ECFC to cross the heavily calcified CTO and the management of entraped RG3 wire with successful retrieval. In predicted difficult, especially heavily calcified, CTO cases, CCTA prior to PCI can be recommended. In our case, the heavy calcification located at ostial to proximal RCA was disclosed by the CCTA, helping us to plan and save the procedure time and radiation doses. Device entrapments during PCI for CTO are complex challenges, requiring the expertise and experience of operators to solve, as the successful solution to the entrapment without complication after a series of interventions in our cases.