
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-070
A Case With Double Chronic Total Occlusion: Between a Rock and a Hard Place
By Weiting Sung, Yi Lin Tsai, You-Ning Chang, Yi-Tsang Fu
Presenter
Weiting Sung
Authors
Weiting Sung1, Yi Lin Tsai1, You-Ning Chang1, Yi-Tsang Fu1
Affiliation
Taipei Veterans General Hospital, Taiwan1,
View Study Report
TCTAP C-070
Coronary - Complex PCI - CTO
A Case With Double Chronic Total Occlusion: Between a Rock and a Hard Place
Weiting Sung1, Yi Lin Tsai1, You-Ning Chang1, Yi-Tsang Fu1
Taipei Veterans General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
This is a 59-year-old man who is a current smoker (0.5 pack per day for 30 years) with past medical history of dyslipidemia. He suffered from STEMI in 2022/3 and the angiography at that time showed triple vessel disease with RCA and LCX CTO. A DES was deployed over LAD-M to -D. Progressive chest tightness (CCS II) was noted so he came to our facility for medical assistance. Physical examinations at the first encounter were normal.
Relevant Test Results Prior to Catheterization
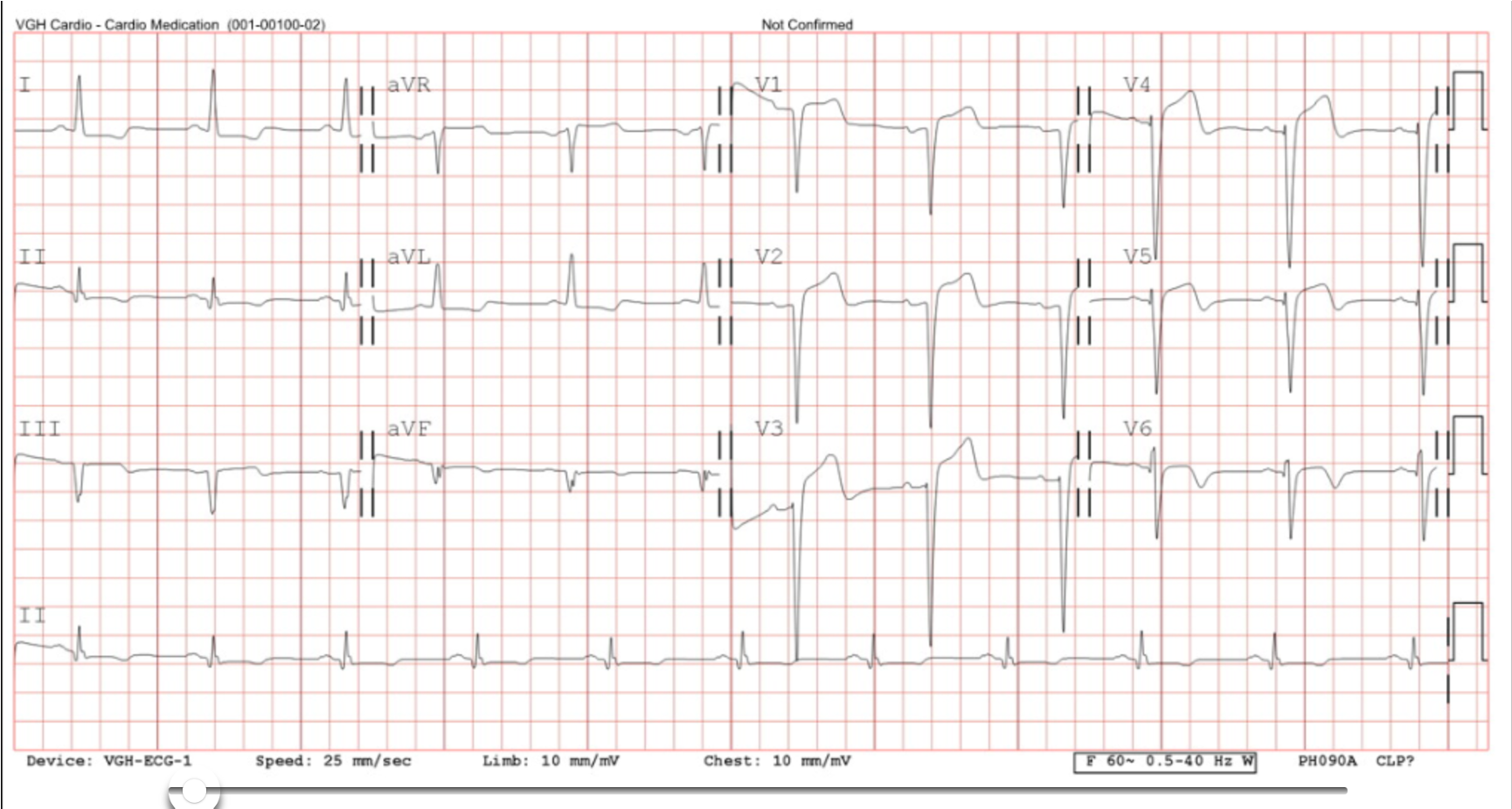
ECG prior to the procedure showed sinus rhythm with left bundle branch block. Echocardiography showed moderately reduced LVEF (32%), and wall motion abnormality seen in septal to posterior wall area.
Relevant Catheterization Findings
Left main: PatentLeft anterior descending artery: -M to -D: instent patentLeft circumflex artery: -M: CTO with auto-collateral circulationRight coronary artery: -M: CTO with septal collateral circulation from LAD, AV groove collaterals from LCX



Interventional Management
Procedural Step
[1st time Procedure: RCA CTO]Dual injection was performed (transradial with JR 4/7 Fr guide catheter(GC) and transfemoral with EBU 3.75/7 GC).A Gaia III guidewire (GW) cannot cross the CTO antegradely with Finecross microcatheter (MC), even using paralle wiring technique via Crusade MC. Sion GW cross the septal collaterals with APT 1.7Fr/150cm MC and reached RCA-M. JR GC was changed to AL 1/7 Fr. A Fielder FC FW crossed the lesion with Corsair Pro MC.IVUS showed eccentric calcified lesion at CTO entry and GW within true lumen.RCA-PL showed TIMI2 but wiring was failed. A DEB was deployed over RCA-PDA as investment PCI. Two DESs were deployed from RCA-P to -D.
[2nd time procedure: LCX CTO]Primary retrograde approach was done transradially with AL 1/7 Fr GC. A Gaia II GW was advanced to RCA-PL and a DES was deployed over RCA-PL. Then, GC with EBU 3.75/7 GC was engaged transfemorally.A SUOH 03 GW was advanced to AV groove collaterals and reached LCX-M with a Craravel MC. However, the MC cannot advance further.Antegrade puncture failed with Conquest pro 12 with Cosair pro MC. Channel dilation was performed at AV groove collaterals with a Ikazuchi 1.0x6mm balloon catheter. The MC was changed to an APT MC and advanced to LCX-M.Reverse CART failed, so we retried kissing wire and advanced a Conquest Pro 12 GW to distal true lumen.IVUS revealed diffuse lesion of LCX and GW within true lumen. A DES was deployed over LCX-P and a DEB was inflated over LCX-D. Final angiography showed TIMI-3 flow

[2nd time procedure: LCX CTO]Primary retrograde approach was done transradially with AL 1/7 Fr GC. A Gaia II GW was advanced to RCA-PL and a DES was deployed over RCA-PL. Then, GC with EBU 3.75/7 GC was engaged transfemorally.A SUOH 03 GW was advanced to AV groove collaterals and reached LCX-M with a Craravel MC. However, the MC cannot advance further.Antegrade puncture failed with Conquest pro 12 with Cosair pro MC. Channel dilation was performed at AV groove collaterals with a Ikazuchi 1.0x6mm balloon catheter. The MC was changed to an APT MC and advanced to LCX-M.Reverse CART failed, so we retried kissing wire and advanced a Conquest Pro 12 GW to distal true lumen.IVUS revealed diffuse lesion of LCX and GW within true lumen. A DES was deployed over LCX-P and a DEB was inflated over LCX-D. Final angiography showed TIMI-3 flow
Case Summary
There are several lessons we learned from this case. First, well-developed retrograde collaterals can be an option for revascularization. In this case, we tried antegrade approach initially for the RCA CTO but failed. Therefore, we choose primary retrograde approach for LCX CTO and crossed the lesion successfully. Secondly, plaque modification may facilitate the success in the subsequent CTO-PCI, like DEB deployment at PDA in this case. Finally, careful balloon dilation at epicardial collateral vessels is feasible if the vessel size is adequate. This may promote the success rate of CTO revascularization.