
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-102
Impella-Assisted Complex High-Risk Percutaneous Coronary Intervention
By Yen-Po Lin, Wen-Lieng Lee
Presenter
Yen-Po Lin
Authors
Yen-Po Lin1, Wen-Lieng Lee1
Affiliation
Taichung Veterans General Hospital, Taiwan1,
View Study Report
TCTAP C-102
Coronary - Complex PCI - Multi-Vessel Disease
Impella-Assisted Complex High-Risk Percutaneous Coronary Intervention
Yen-Po Lin1, Wen-Lieng Lee1
Taichung Veterans General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
The 69-year-old male businessman with pasthistory of type 2 diabetes mellitus, chronic kidney disease stage 3, CAD-TVD statuspost CABG in 2013/05. He suffered from intermittent chest pain for one day andwas diagnosed of acute coronary syndrome with cardiogenic shock in 2023/05. After balloon angioplasty at middle rightcoronary artery at the referring hospital, the patient gotstabilized. He was referred to our hospital for complete percutaneouscoronary intervention.
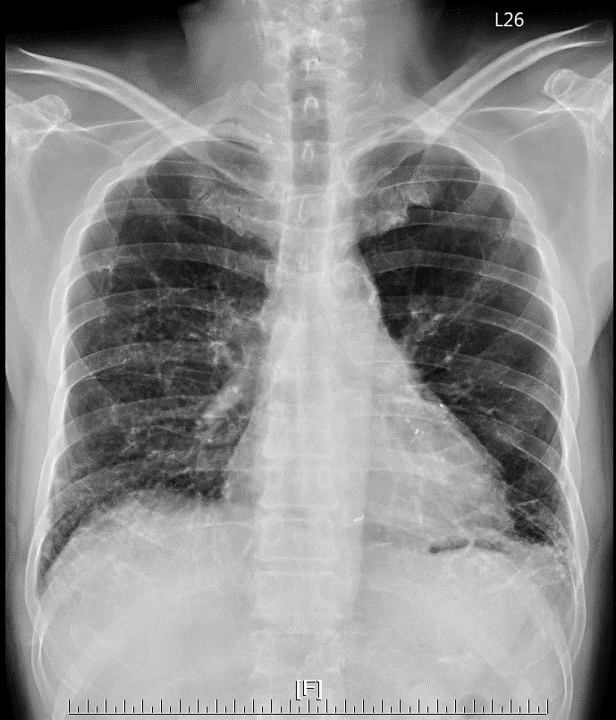
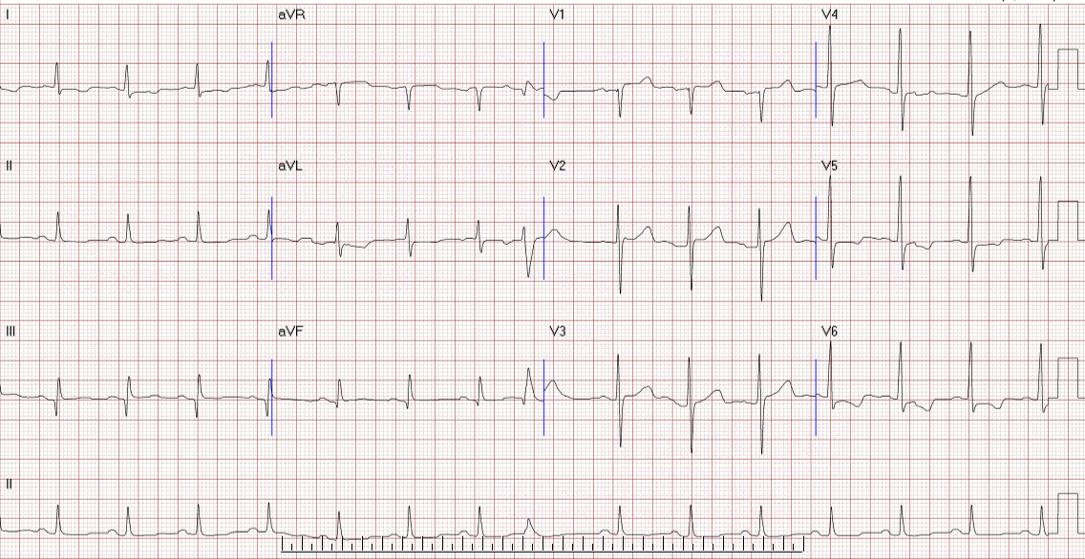
Relevant Test Results Prior to Catheterization
EKG revealed normal sinus rhythm with V5-6 ST segment depression. Chest x-ray showed bilateral lung increased infiltration. Lab data revealed elevated creatinine level to 1.46mg/dl.
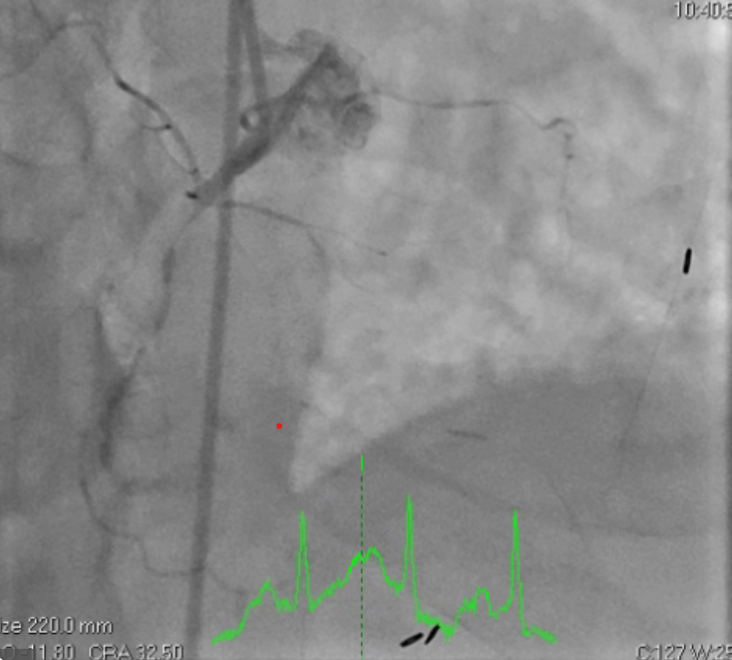
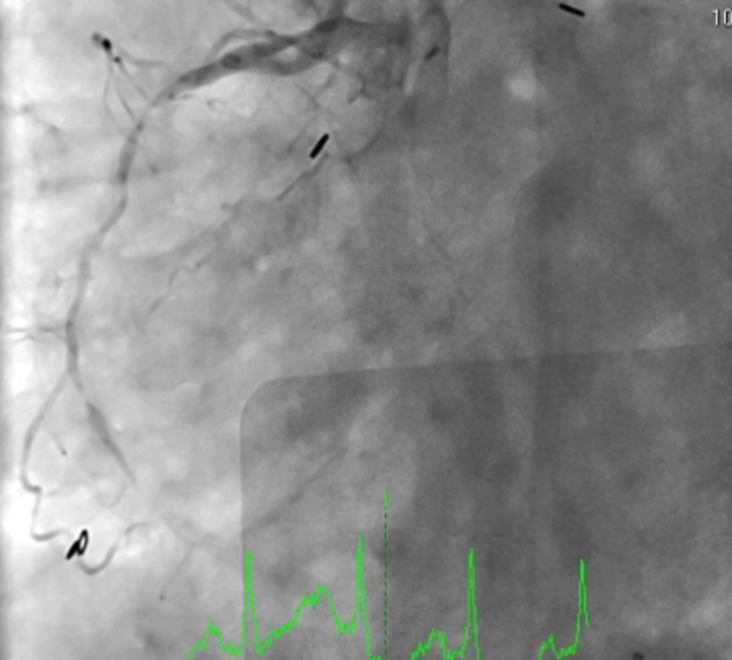
Relevant Catheterization Findings
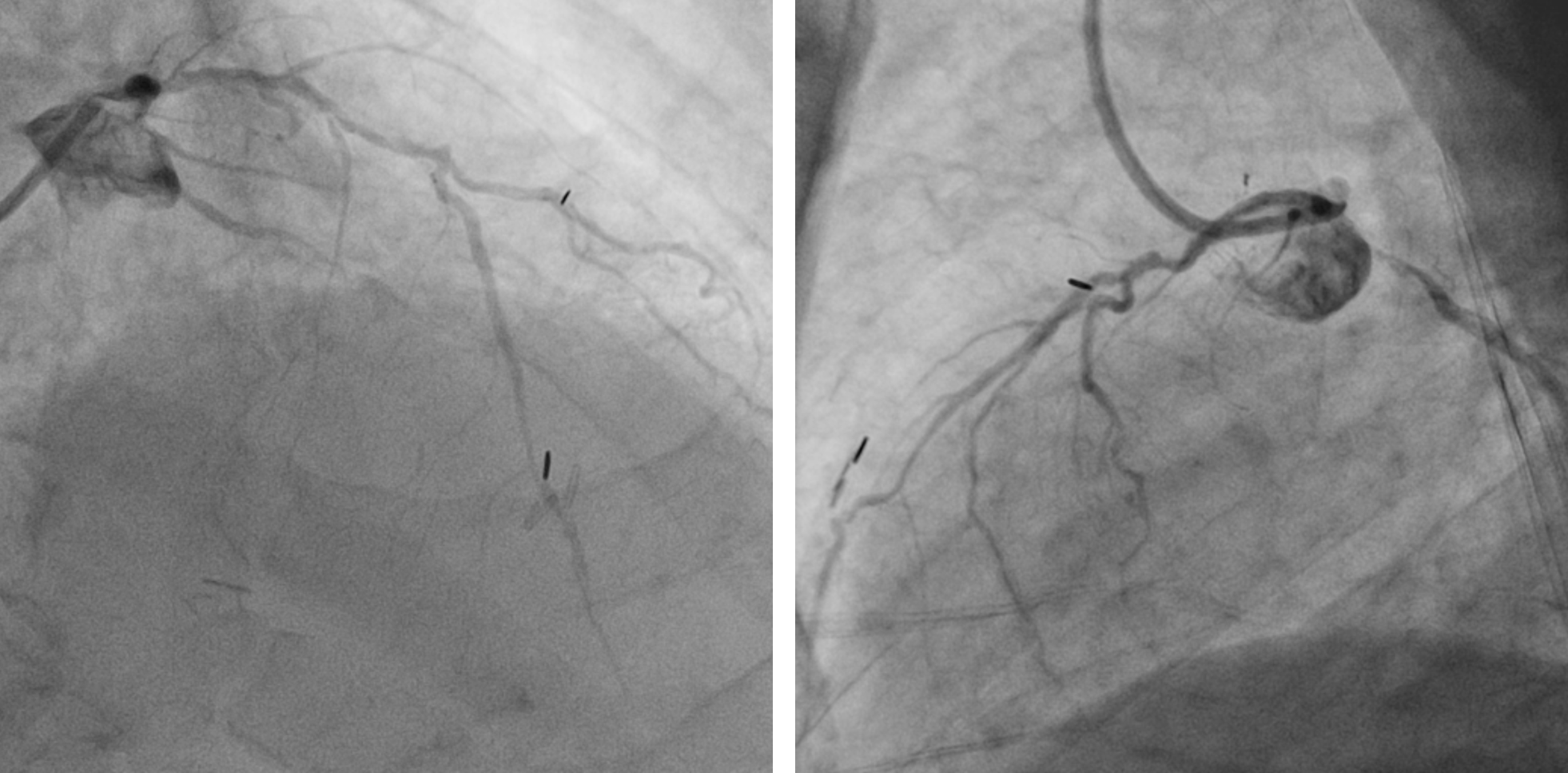
The right coronary artery has severe atherosclerosischanges and thick rotating calcification all the way from ostium to the RCA-PL, 90% stenosis with TIMI II flow down to RCA-PL. 90% ostial stenosisfollowed by diffuse 70% stenosis in the whole left main coronary artery. There arediffuse atherosclerosis changes with heavy eccentric and rotatingcalcification, 60-80% stenosis on LAD. LCX also surrounded by diffuse atherosclerosischanges, heavy calcification and 95% stenosis at ostium.

Interventional Management
Procedural Step
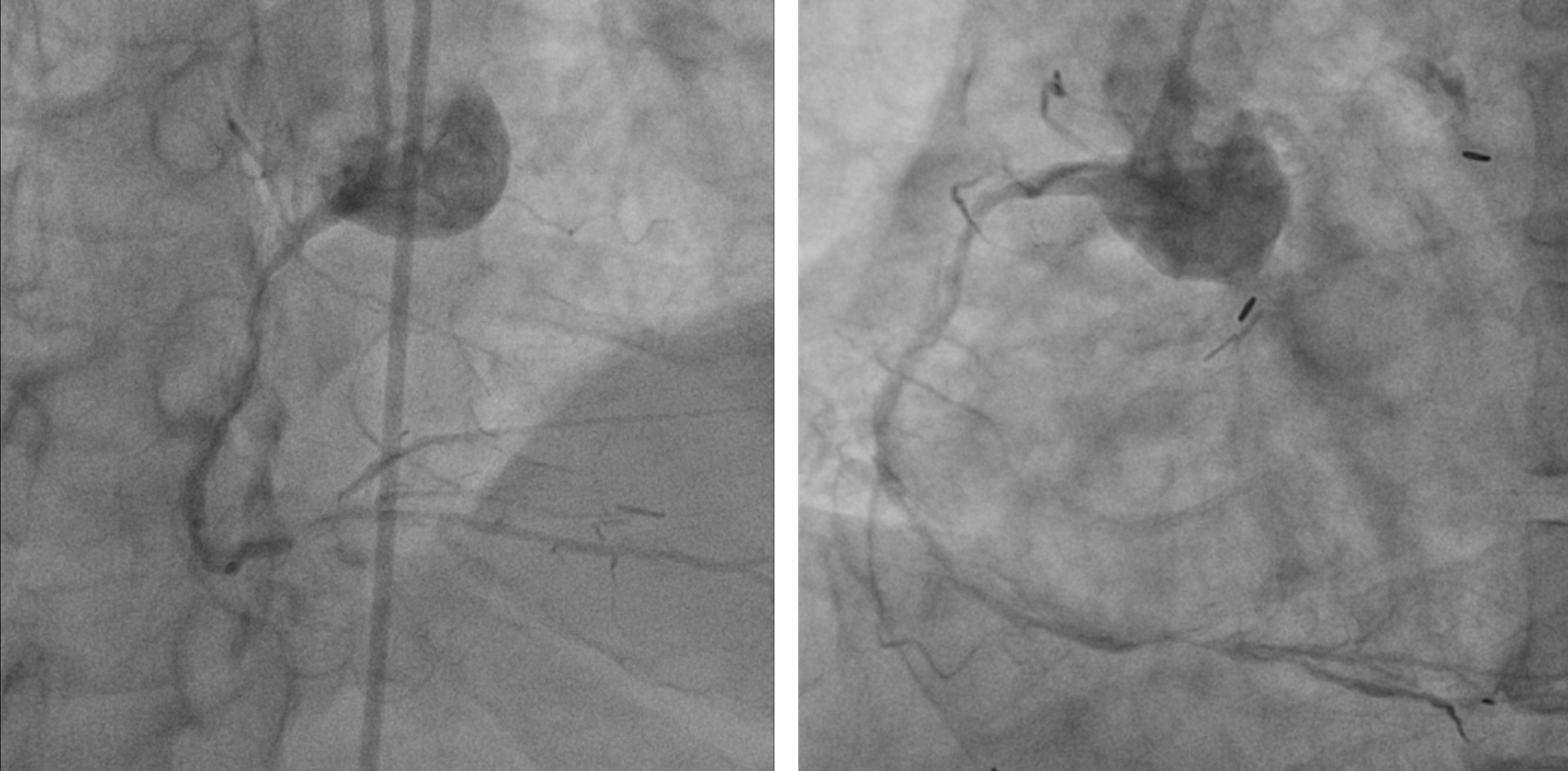
Due to complex anatomies in left coronaryartery and diffuse lesions in the right coronary artery which are notmanageable in this stage, Impella (Abiomed, U.S.) was needed for hemodynamic support. A14Fr sheath could not be advanced through the heavily calcified common iliacartery (CIA). To avoid damage of Impella, CIA was treated with intravascular lithotripsy(Shockwave Medical, U.S.). Impella was advanced without any difficulty.


Case Summary
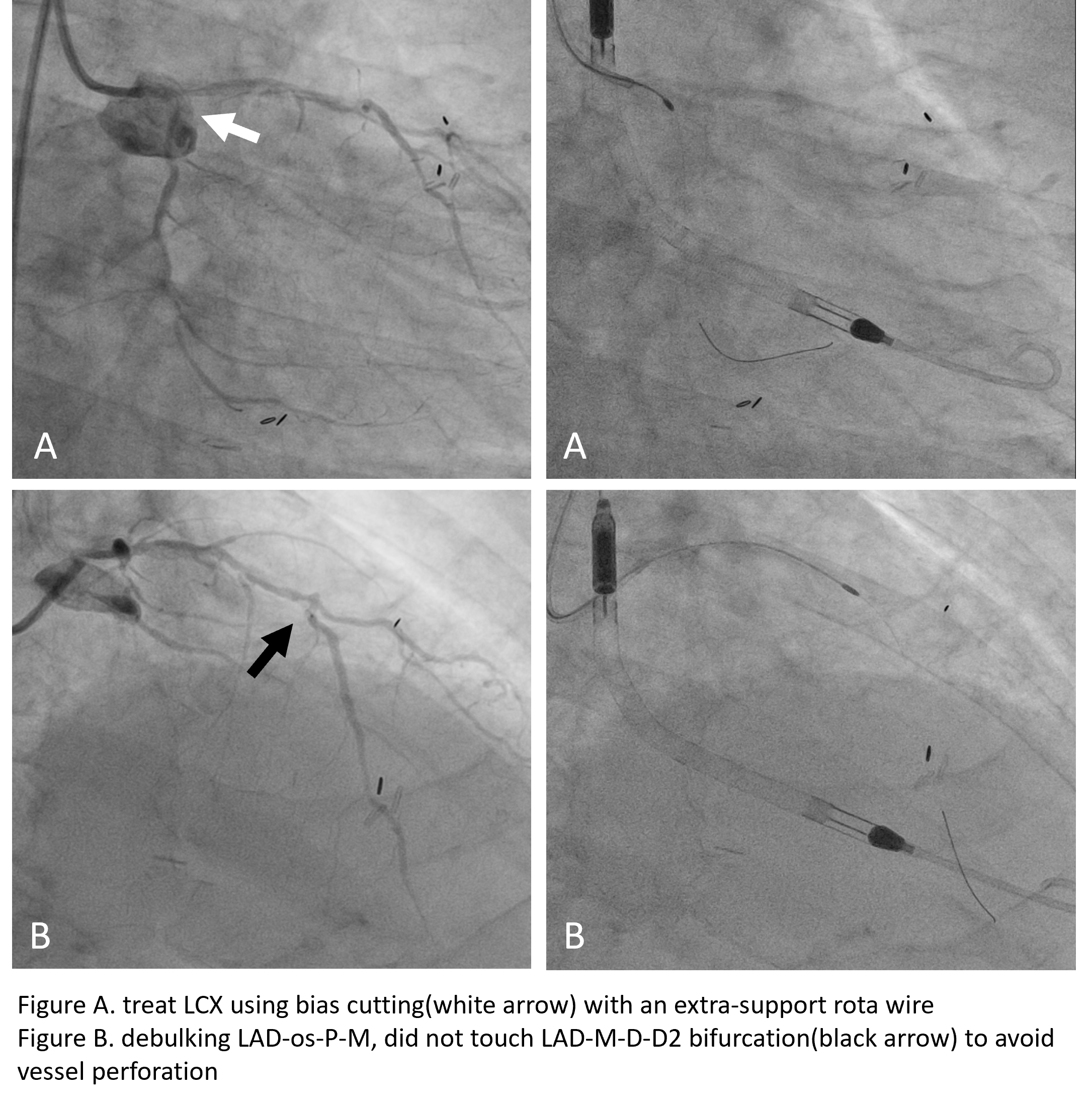
The Impella provided adequate hemodynamic support during high-risk PCI. We should avoid bailout use mechanical support. On the other hand, if we rotablate exactly where needed, we can avoid troubles.