
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-176
What Lies Beneath
By Rowina Lynne Murray, Ahmad Khairuddin Mohamed Yusof, Mohd Tawfeq Mohd Noor, Sharimila Shanmugam, Si Ling Soh, Aslannif Roslan
Presenter
Rowina Lynne Murray
Authors
Rowina Lynne Murray1, Ahmad Khairuddin Mohamed Yusof1, Mohd Tawfeq Mohd Noor1, Sharimila Shanmugam1, Si Ling Soh2, Aslannif Roslan1
Affiliation
National Heart Institute, Malaysia1, National Heart Institute, Malaysia, Malaysia2,
View Study Report
TCTAP C-176
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
What Lies Beneath
Rowina Lynne Murray1, Ahmad Khairuddin Mohamed Yusof1, Mohd Tawfeq Mohd Noor1, Sharimila Shanmugam1, Si Ling Soh2, Aslannif Roslan1
National Heart Institute, Malaysia1, National Heart Institute, Malaysia, Malaysia2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
We present a 63 year old gentleman with percutaneous coronary intervention to LAD in 2005 and RCA in 2019. He was seen in clinic with exertional chest pains which is relieved with rest. He has underlying diabetes, dyslipidemia and is NYHA class 1. He had a tech scan prior to his angioplasty of RCA in 2019 which showed ischemia over the LAD territory. No angioplasty was performed on LAD despite ischemia on functional testing as visually there was only mild ISR.

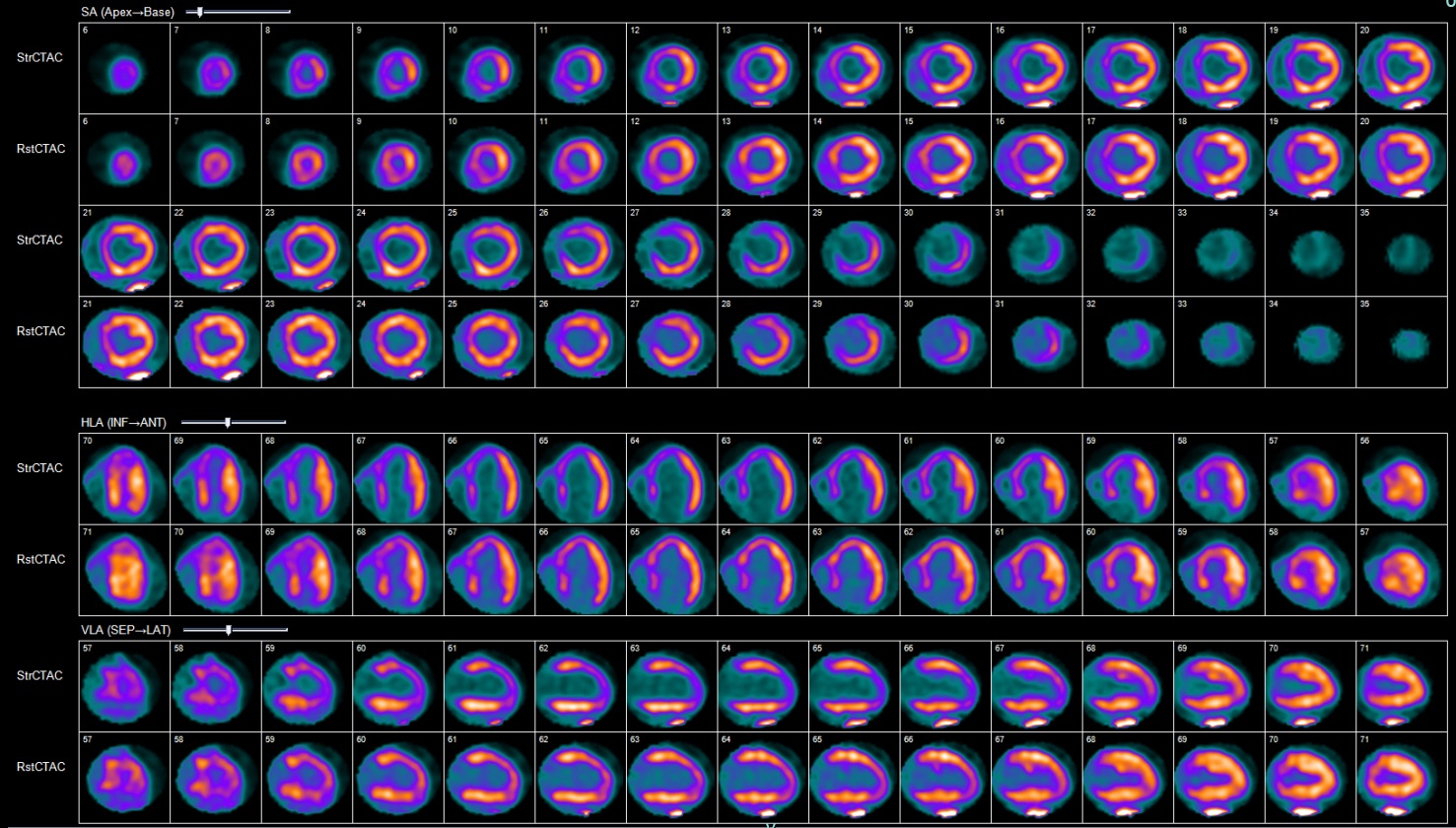
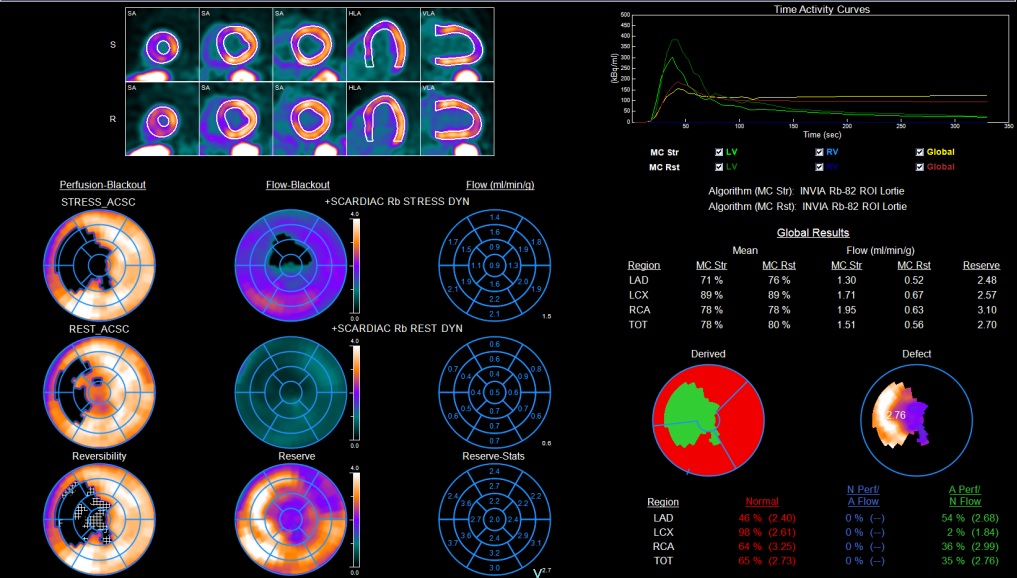
Relevant Test Results Prior to Catheterization
PET CT Perfusion showed moderate ischemia over the LAD territory. Coronary flow reserve of LAD was normal (2.48) suggesting likelihood of macrovascular ischemia. Ejection fraction was 39% at stress and 41% at rest. This is consistent with the transthoracic echocardiography findings.
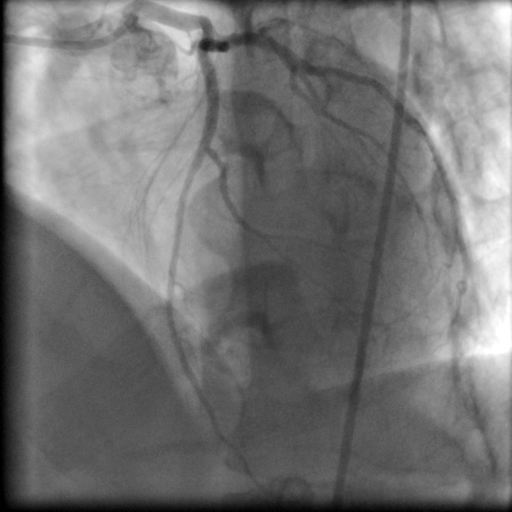
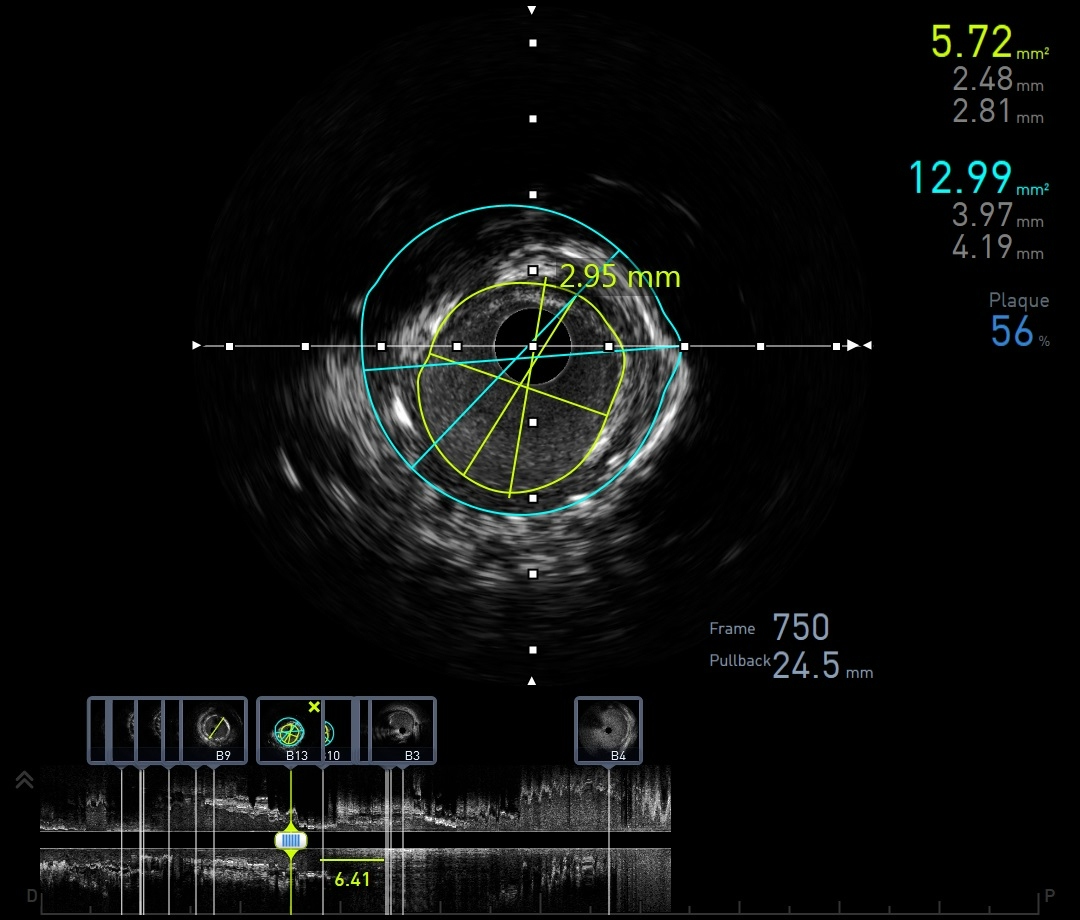
Relevant Catheterization Findings
Coronary angiogram showed slow flow through the previous LAD stent with no significant ISR. Due to the slow flow and discrepancy between degree of ISR and PET CT finding we decided to image the lesion with IVUS which revealed that the previous stent was under expanded. The previous stent size was 3.0 mm but measurement of vessel size is 3.5mm. This produced an MSA of 5.72 mm2

Interventional Management
Procedural Step
The lesion was predilated with a 3.5/15mm normal balloon at 22 atm. TIMI III flow was restored immediately after predilation. A paclitaxel drug coated balloon (3.5/15mm) was applied to proximal and mid stent at 8 atm (nominal pressure 6 atm) with a 1:1 ratio to lesion preparation. IVUS was deployed again to evaluate the final results which shows good stent expansion and apposition with a MSA of 9.14mm2. Good angiographic results attained post balloon and patient was asymptomatic and remained hemodynamically stable throughout.

Case Summary
This case illustrates the importance of multimodality assessment of lesion severity. This patient had symptoms since 2019 where the technetium scan had already demonstrated ischemia in the LAD territory. As the LAD stent showed mild ISR and there was an angiographically significant RCA lesion, PCI was done to RCA instead. Back in 2019 the utilization of PET CT and IVUS was not yet mainstream and operators rely on visual determination of severity which can be misleading. Corroborating information from the PET CT in localization of ischemia and flow reserve, we were alerted of the need to further evaluate the LAD stent instead of visually assessing stent patency as a mark of adequate perfusion