
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-037
Leopard Crawl Technique in Retrieval of Entrapped Side Branch Wire in Calcified, Bifurcation Lesion
By Neerusha Kaisbain, Chong Wei Loong, Chew Fui Lo, Khoo Song Weng Ryan, Houng Bang Liew
Presenter
Neerusha Kaisbain
Authors
Neerusha Kaisbain1, Chong Wei Loong2, Chew Fui Lo1, Khoo Song Weng Ryan1, Houng Bang Liew1
Affiliation
Queen Elizabeth II Hospital, Malaysia1, KPJ Sabah Specialist Hospital, Malaysia2,
View Study Report
TCTAP C-037
Coronary - Complex PCI - Calcified Lesion
Leopard Crawl Technique in Retrieval of Entrapped Side Branch Wire in Calcified, Bifurcation Lesion
Neerusha Kaisbain1, Chong Wei Loong2, Chew Fui Lo1, Khoo Song Weng Ryan1, Houng Bang Liew1
Queen Elizabeth II Hospital, Malaysia1, KPJ Sabah Specialist Hospital, Malaysia2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
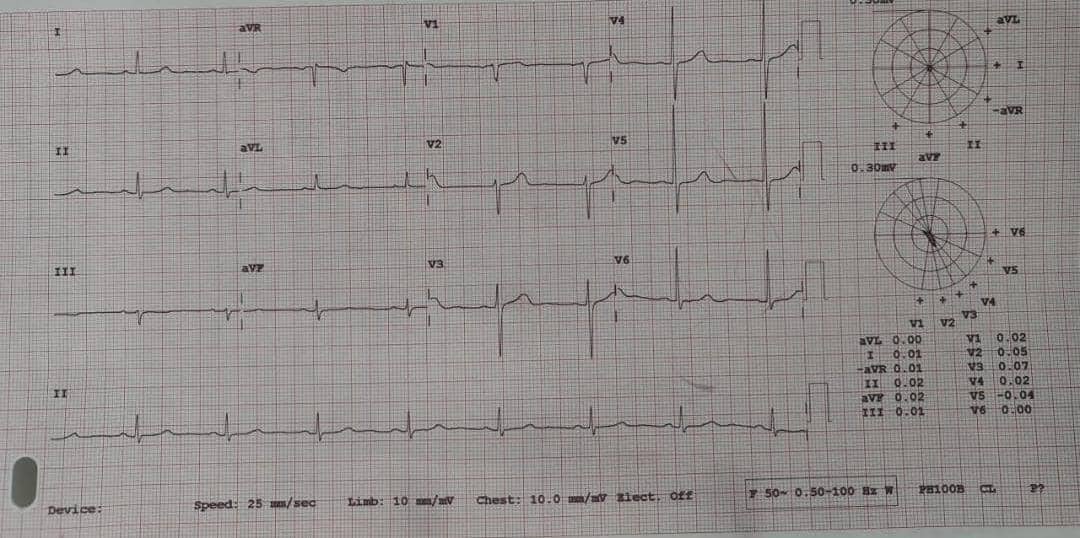
A 70 years old lady with diabetes mellitus, hypertension, dyslipidaemia, has been having effort angina of Canadian Cardiovascular Society (CCS) class II for a year. The physical examination showed no relevant clinical findings. The ECG was showed sinus rhythm with no ischemic changes.
Relevant Test Results Prior to Catheterization
A transthoracic echocardiography showed normal left ventricular ejection fraction with no regional wall motion abnormalities. She underwent treadmill exercise stress test, which was positive. She had history of percutaneous coronary intervention done to the right coronary artery three months prior and the left anterior descending artery was planned for a staged procedure.

Relevant Catheterization Findings
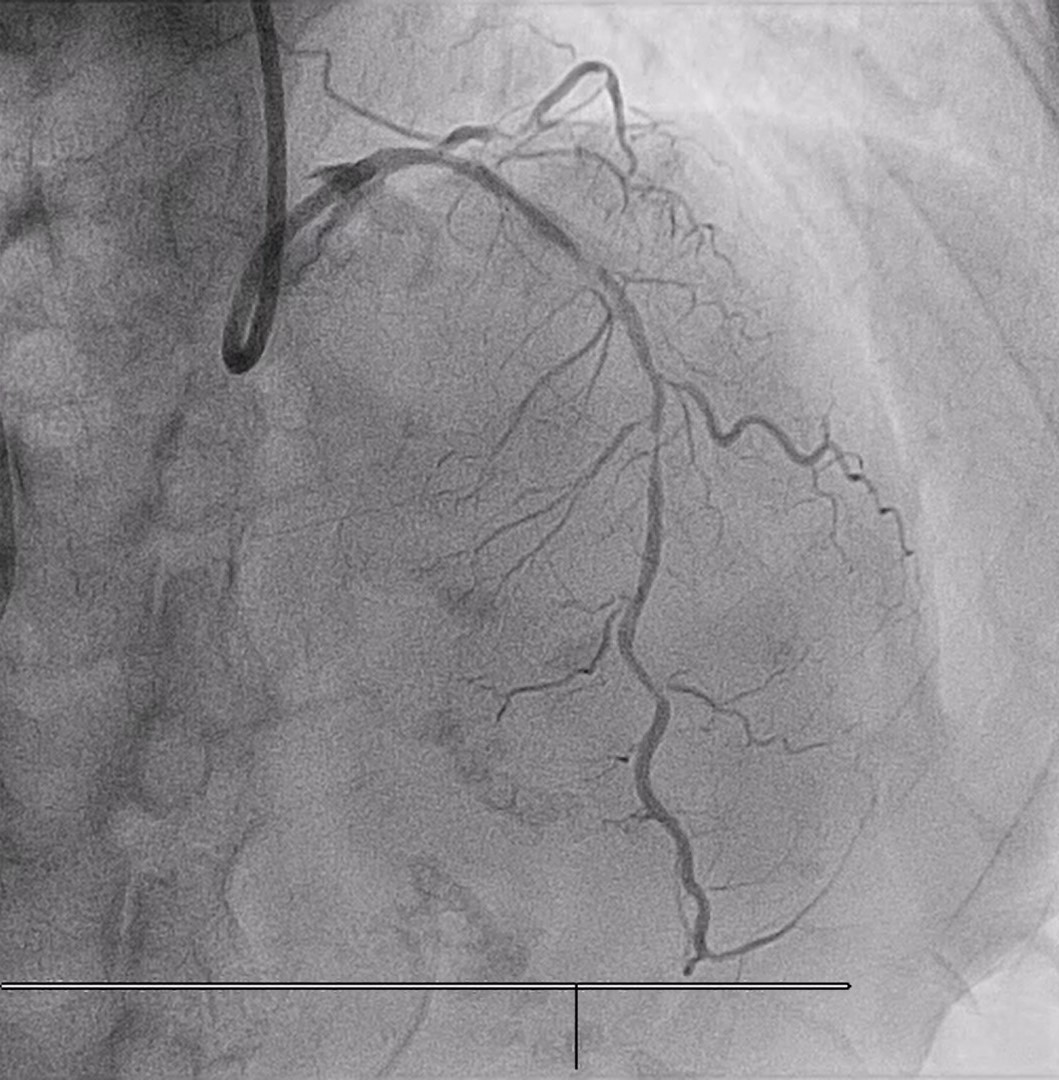
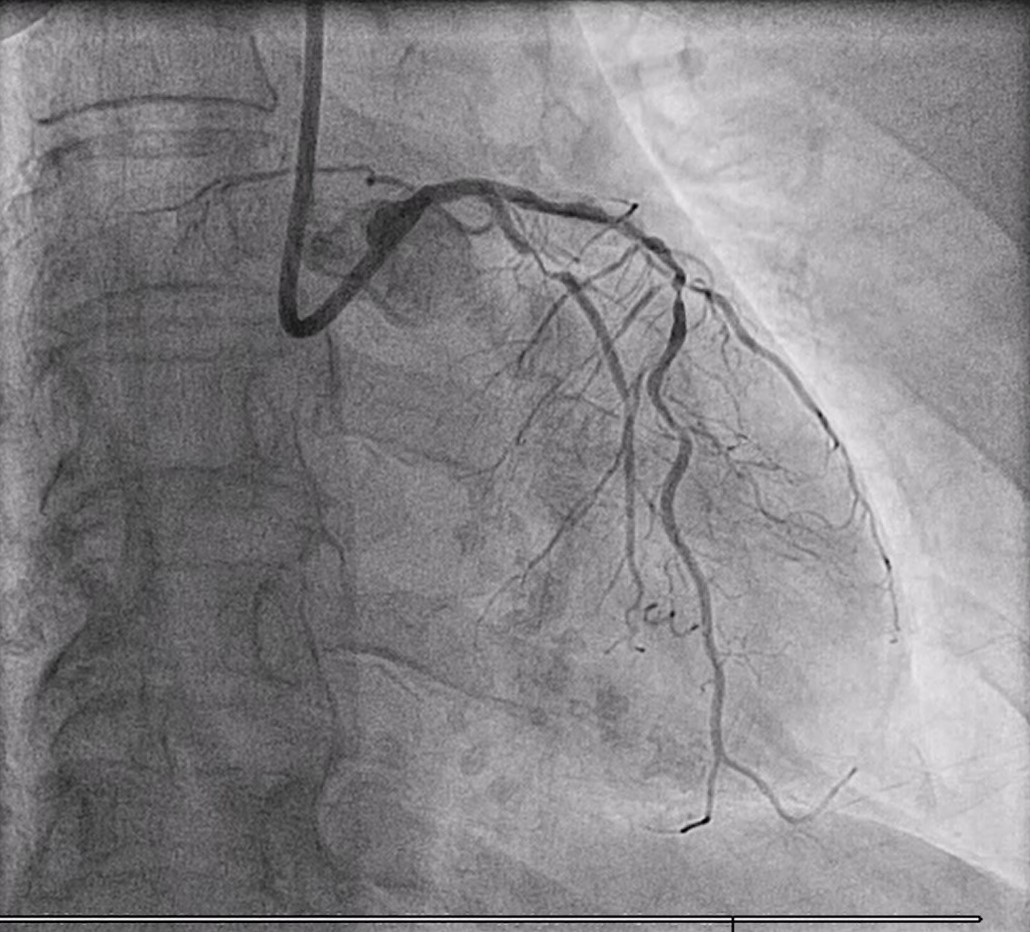
Coronary angiography revealed a dual vessel disease. The left main stem had moderate tubular disease. The left anterior descending artery (LAD) was calcified, proximal and mid 90% disease, involving the main diagonal with Medina classification 1,1,1. The left circumflex (LCx) was non dominant, proximal 90% disease. The previously treated RCA segment was patent with mild residual disease.
Interventional Management
Procedural Step
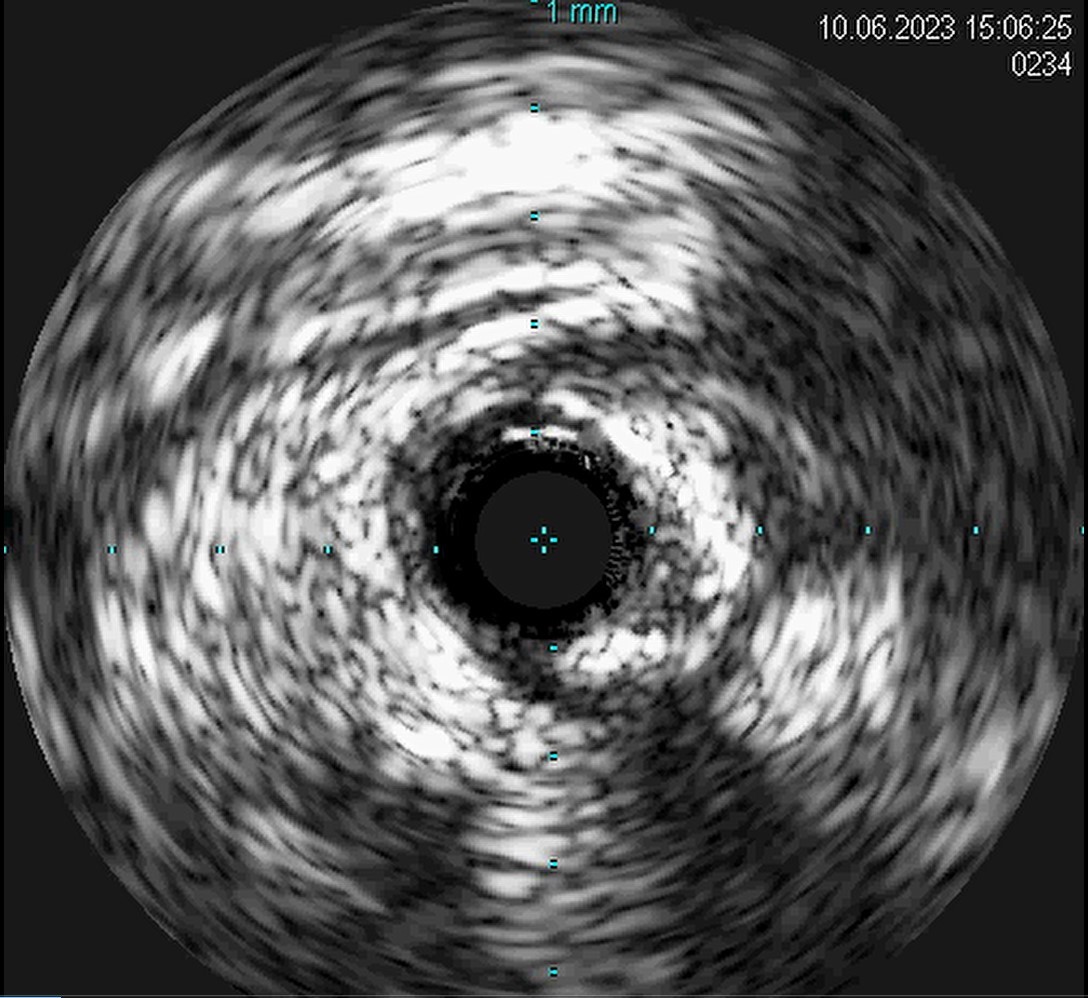
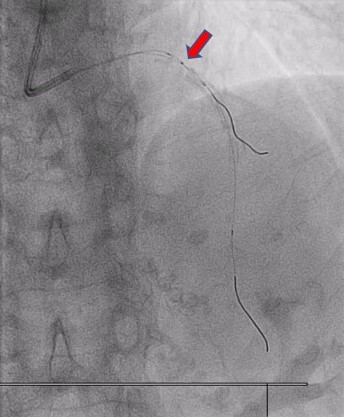
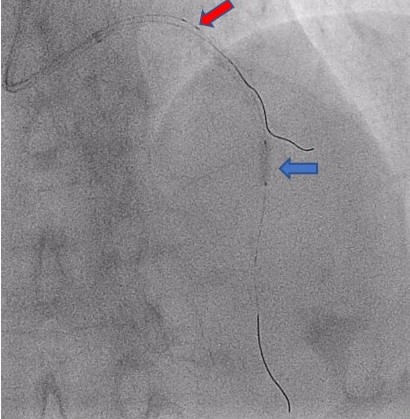
Staged PCI of the LAD was done via a trans radial approach using a 7 Fr radial sheath and a 7 Fr EBU 3.5 guiding catheter. A workhorse guidewire and a Finecross microcatheter was passed into the distal LAD. The guidewire was exchanged to ROTAWIRE™ Drive and Rotablation was done with 1.5 burr with 160k RPM for 5 runs. In view of Medina 1,1,1 bifurcation lesion, we decided to protect the main diagonal branch with BMW guidewire. Intravascular Ultrasound (IVUS) showed heavy calcification with calcium nodule. The proximal to distal LAD lesion was further predilated with scoring and non-compliant balloons with good balloon expansion. The distal LAD lesion is treated with drug coated balloon2.25 x 40 mm. The proximal to mid LAD lesion was stented with 2.75 x 33 mm drug eluting stent, deployed at 14 atm. After stenting however, the main diagonal branch wire was trapped. A firm traction of the diagonal wire was unsuccessful in its removal. An attempt to advance the microcatheter outside the stent strut to release the trapped segment failed. The microcatheter was removed and a semi-compliant (SC) 0.85 x 10 mm balloon was advanced abluminally in leopard crawl technique. However, it failed to advance further. An SC balloon 2.5x 15 mm was inflated at the mid LAD as an anchor for extra support and another shorter 0.85 mm SC balloon of 5mm was passed abluminal to the stent with leopard crawl method and the diagonal wire was successfully released from the trapped segment and retrieved.

Case Summary
Entrapped guidewire is a common complication of percutaneous coronary intervention, especially in high risk lesions such as calcification.