
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-170
Debulking Calcium Nodule With Orbital Atherectomy
By Jieli Kua, Poay-Huan Loh
Presenter
Jieli Kua
Authors
Jieli Kua1, Poay-Huan Loh2
Affiliation
Mount Elizabeth Orchard Hospital, Singapore1, National University Heart Centre, Singapore2,
View Study Report
TCTAP C-170
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
Debulking Calcium Nodule With Orbital Atherectomy
Jieli Kua1, Poay-Huan Loh2
Mount Elizabeth Orchard Hospital, Singapore1, National University Heart Centre, Singapore2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
64 year old gentleman who is a non smoker and has a significant past medical history of hypertension and hyperlipidemia. He presented to our clinic with symptoms of angina for the last few weeks. Physical examination was unremarkable.
Relevant Test Results Prior to Catheterization
CT coronary angiogram was performed showing calcium score of 3247 and triple vessel disease. Echocardiogram showed normal ejection fraction and no significant valvular function.
Relevant Catheterization Findings
Coronary angiogram showed middle left main 30%, middle left anterior descending artery 80%, distal left anterior descending artery 80%, middle right coronary artery 80%, right posterior descending artery 90% and right posterolateral artery 80%. We proceeded with angioplasty of the LAD and for staged procedure of the right coronary artery. The mid LAD was stented with a 2.5 x 23 mm drug eluting stent and the distal LAD treated with 2 x 30 mm drug coated balloon.



Interventional Management
Procedural Step
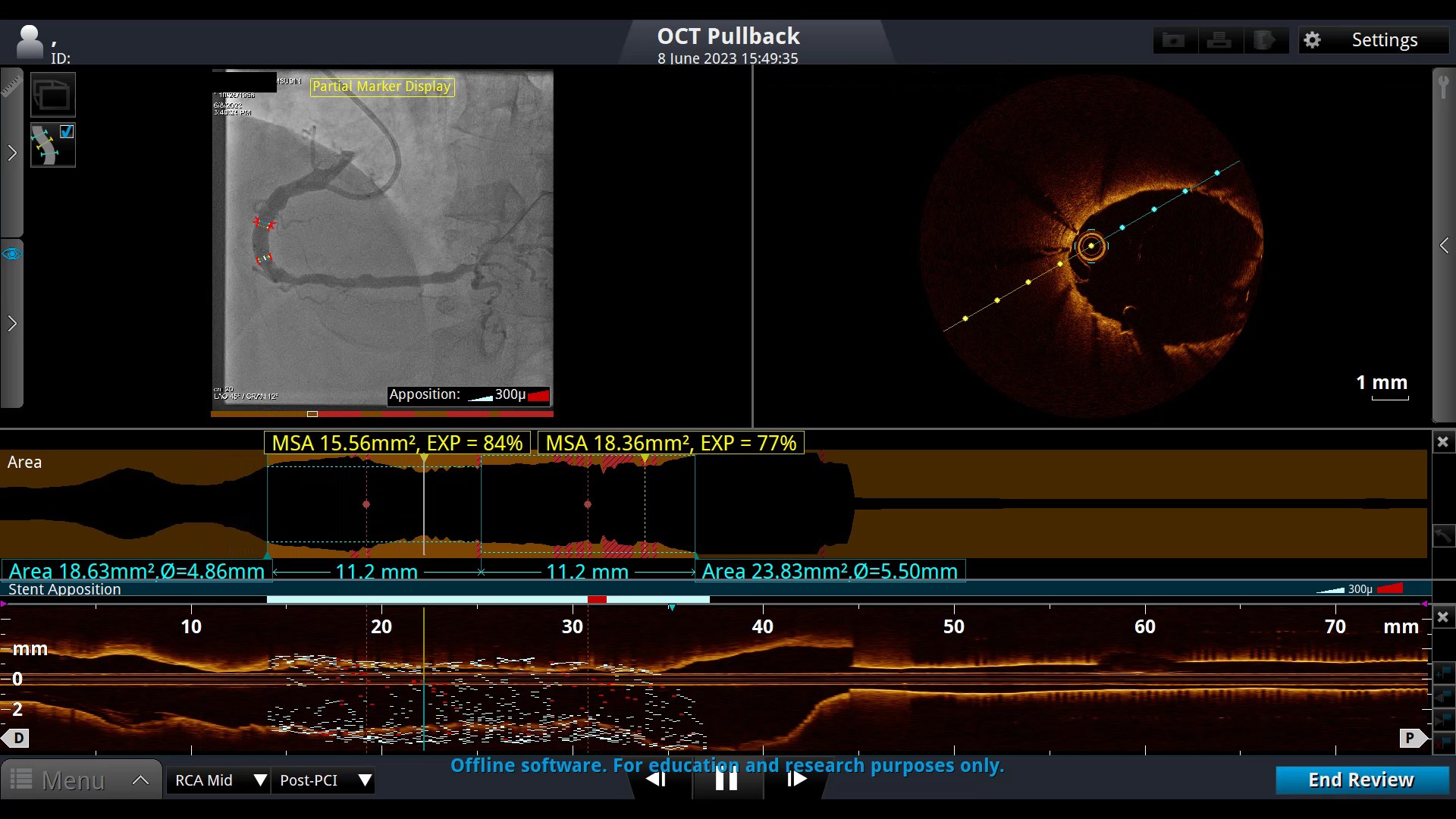
We performed angioplasty of the RCA via the right radial approach with a 6 French sheath. 6 Fr AL 1 guide catheter to RCA and a Runthrough NS wire used to cross the lesion. Dragonfly OCT catheter pullback shows calcified nodule with a MLA of 1.64 mm2. Exchanged to Viper stiff wire with Mizuki microcatheter. We performed 6 runs of orbital artherectomy at low speed with Diamondback Orbital device and then 6 runs at high speed. Repeat OCT shows improvement in MLA to 2.81 mm2. We then predilated with w Wolverine 4 x 15 mm cutting balloon and a Sapphire 4.5 x 15 mm NC balloon. Repeat OCT now shows improved MLA to 6.41 mm2. A Synergy Megatron 5 x 20 mm DES stent was deployed across the lesion and this was post dilated with a Sapphire 5 x 12 mm NC balloon. Repeat OCT run shows good area expansion with a distal MSA of 15.56 mm2 and proximal MSA of 20.33 mm2. Final angiogram good results.


Case Summary
Calcified nodules are associated with poor stent expansion and elliptical shaped stents post stenting. Orbital atherectomy maybe a good treatment tool for such lesions as nodule debulking prior to stent deployment improves stent expansion.