
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-139
REGRET ME NOT: A Case of Stentablation Using Halfway Rotational Atherectomy of an Underexpanded and Undilatable Coronary Artery Stent in a Patient With a Recent ST-Elevation Myocardial Infarction.
By Allan Jake Cabanban Dela Cruz, Jhoanna Marcelo
Presenter
Allan Jake Cabanban Dela Cruz
Authors
Allan Jake Cabanban Dela Cruz1, Jhoanna Marcelo1
Affiliation
Philippine Heart Center, Philippines1,
View Study Report
TCTAP C-139
Coronary - Complication Management
REGRET ME NOT: A Case of Stentablation Using Halfway Rotational Atherectomy of an Underexpanded and Undilatable Coronary Artery Stent in a Patient With a Recent ST-Elevation Myocardial Infarction.
Allan Jake Cabanban Dela Cruz1, Jhoanna Marcelo1
Philippine Heart Center, Philippines1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 70 year-old Filipino, Male, Married, Bus Driver with uncontrolled hypertension and no family history of cardiovascular disease came in at the emergency room department with a chief complaint of sudden onset of a persistent 9/10 typical anginal pain with associated diaphoresis. Patient had the following vital signs: BP = 150/90 mmHg, HR = 83 bpm, RR = 20 cpm, Temp = 36.7o C, spo2 = 98% at room air. Patient had an unremarkable physical examination findings.

Relevant Test Results Prior to Catheterization
A 12 Lead Electrocardiogram (Fig 1.0) was immediately done within 10 minutes upon arrival at the emergency room department and revealed a sinus rhythm with normal axis, a left ventricular hypertrophy with an ST-Elevation in leads V1-V4. His cardiac high sensitivity troponin-I was elevated at 30,556 ng/L. Consent was obtained for an emergency coronary angiogram with possible percutaneous coronary intervention. Creatinine was at 0.12 mmol/L with an eGFR of 56.1 mL/min/1.73m2

Relevant Catheterization Findings
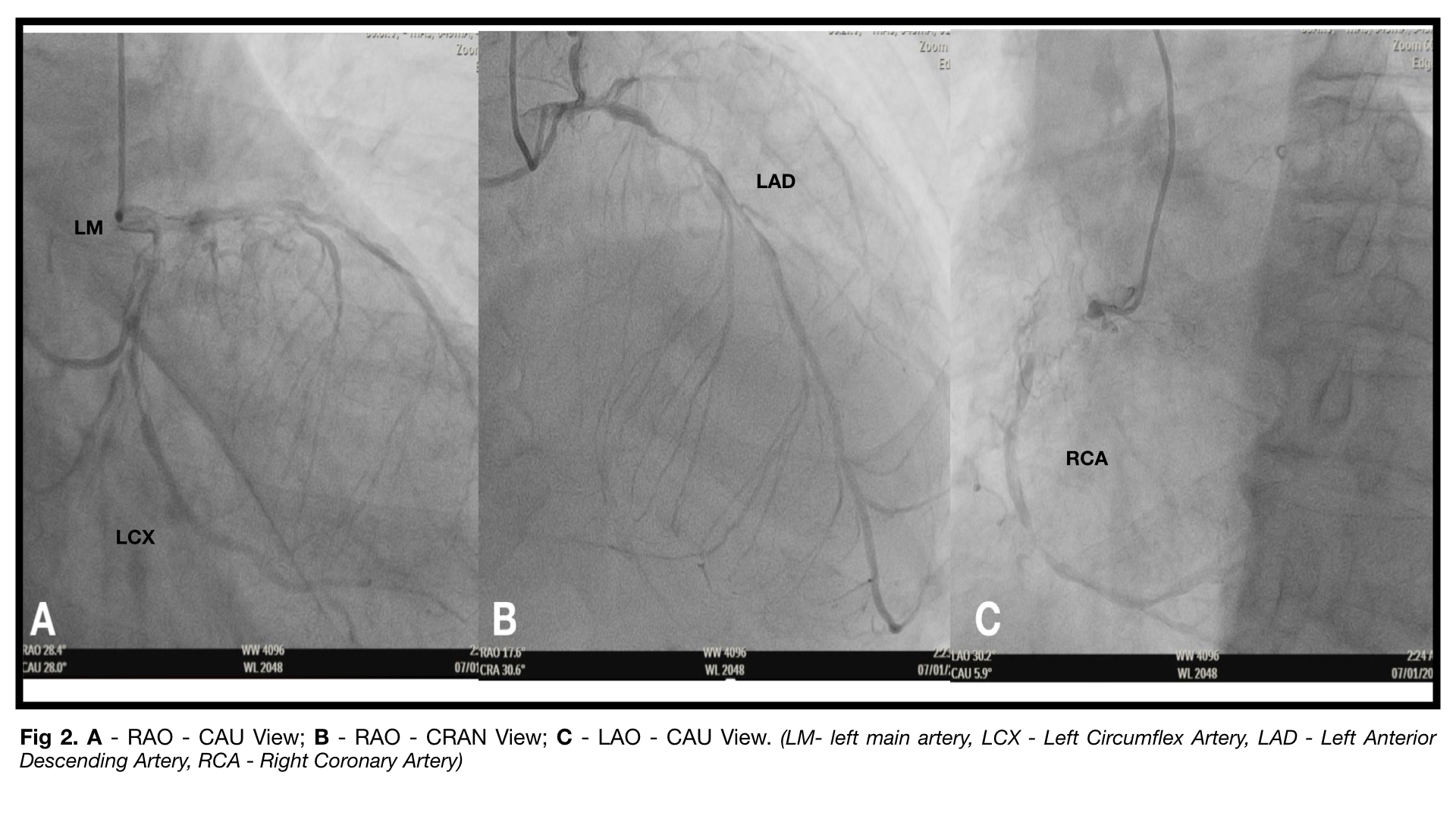
Coronary Angiogram via right radial approach using a 5F TIG catheter revealed a severe three vessel disease without left main involvement. The LAD is a fair sized type III vessel which is diffusely diseased with tightest lesion at 80% at its proximal to mid segment. The LCX is a fair-sized diseased vessel with tightest lesion at its distal segment at 80%-90%. There is a chronic total occlusion of the RCA with its mid to distal branches seen via bridging collaterals and left to right collaterals.
Interventional Management
Procedural Step
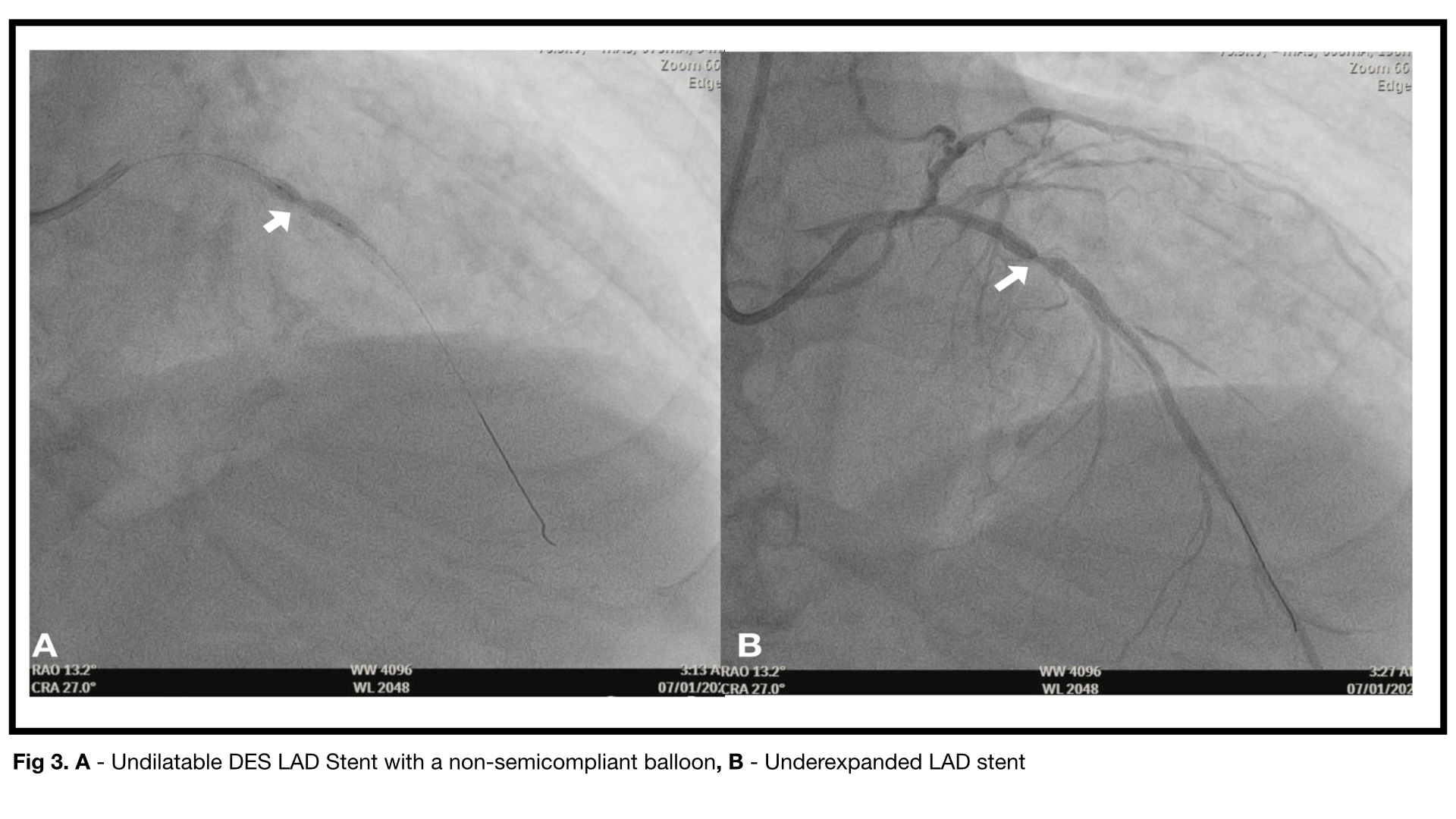
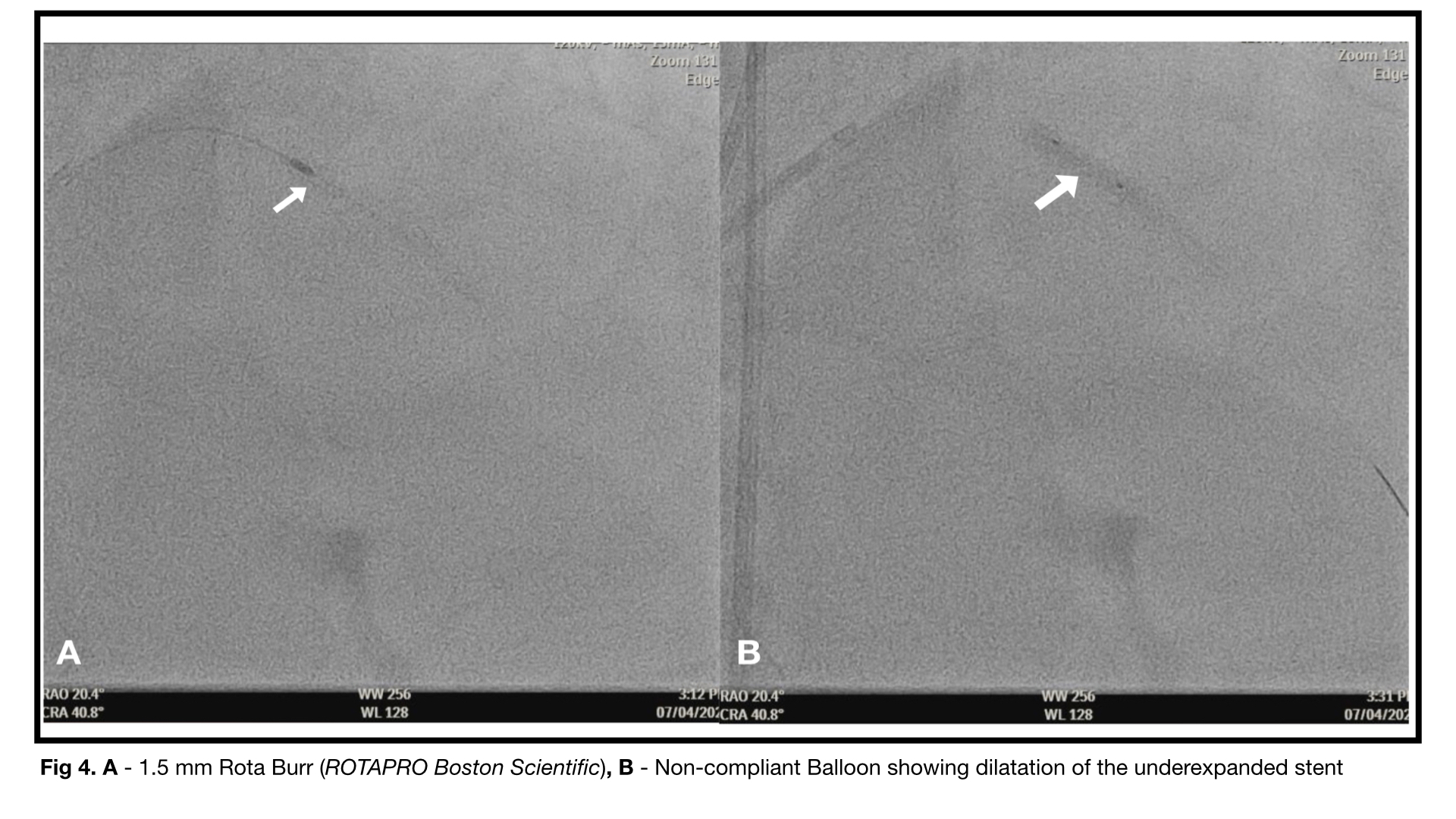
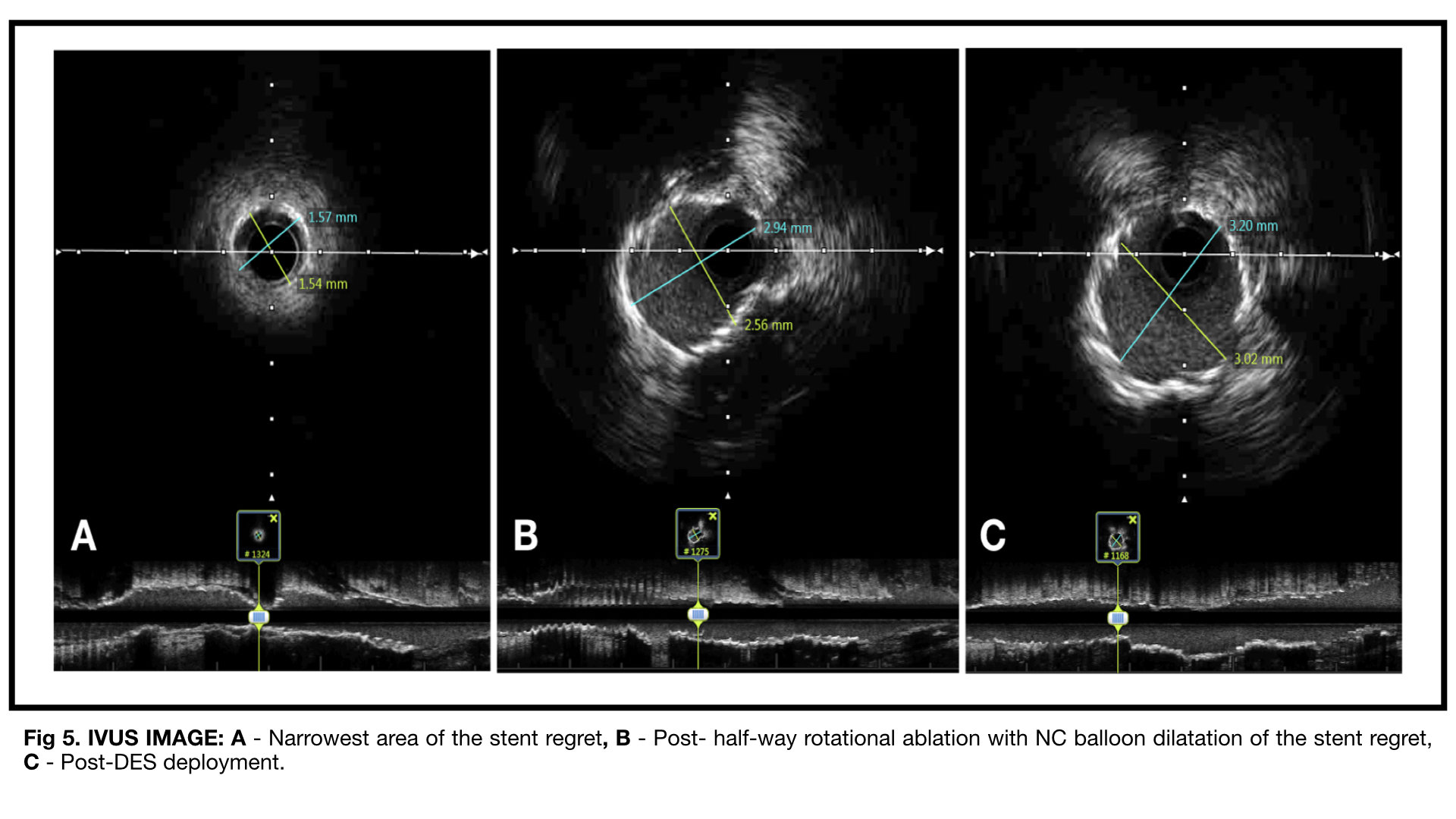
After the primary PCI of the culprit artery, an undilatable and underexpanded stent was evident. After 72 hours of conservative management and careful planning, a complex PCI of the RCA-CTO lesion, a rotational ablation of the underexpanded stent and provisional stenting strategy of the LCX with on-site surgical back up was carried out. A dual femoral access using 7F VL and 7F JR (Mach 1 Boston Scientific) were used. IVUS was done for burr size determination (> 0.6 artery to burr ratio using imaging). IVUS showed a 1.57 x 1.57 mm diameter with an MLA of 1.60 mm2 at the narrowest area of the underexpanded stent. A 1.5 mm burr (RotaLink Pro) was used with an ablation speed of 180,000 rpm with short runs of less than 15 seconds. After 7 runs, a resistance was evident and subsequent burr entrapment. The rota burr was carefully withdrawn via manual traction with Dynaglide to prevent burr head breakdown while preventing passive engagement of the guide catheter. De-escalation to smaller burr was contemplated but a repeated high pressure balloon inflations at rated burst enabled expansion of the partially ablated stent. IVUS run after stent ablation showed sparse stent struts with an area of 2.6mm2. A drug eluting stent was then position distal to the ablated area to cover the denuded parts and overlap with the proximal part of the first stent upto the ostium of the LAD with TIMI grade 3 flow and IVUS run showed well apposed stents with MSA of 3.0 mm2 (100% expansion).
Case Summary
Stentablation by rotational atherectomy has been reported as an option to correct underexpanded stents. However, excessive stent damage, distal embolization of metal particles, excessive heat generation, and burr entrapment remains a concern for operators. Stentablation using Half-way rotational atherectomy is generally safe and effective as a bail-out procedure to correct stent regret. Intravascular imaging should be utilized when performing rotational atherectomy for stent ablation to guide burr size, determine extent of areas to ablate and stent size selection post-ablation.