
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-085
In-Stent Restenosis Stenting by Optical Coherence Tomography Guidance
By Dr Raja Ramesh Nukavarapu, Ramesh Babu Pothineni
Presenter
Dr Raja Ramesh Nukavarapu
Authors
Dr Raja Ramesh Nukavarapu1, Ramesh Babu Pothineni2
Affiliation
Aster Ramesh Hospital, India1, Aster Ramesh Hospitals, India2,
View Study Report
TCTAP C-085
Coronary - Complex PCI - In-Stent Restenosis
In-Stent Restenosis Stenting by Optical Coherence Tomography Guidance
Dr Raja Ramesh Nukavarapu1, Ramesh Babu Pothineni2
Aster Ramesh Hospital, India1, Aster Ramesh Hospitals, India2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
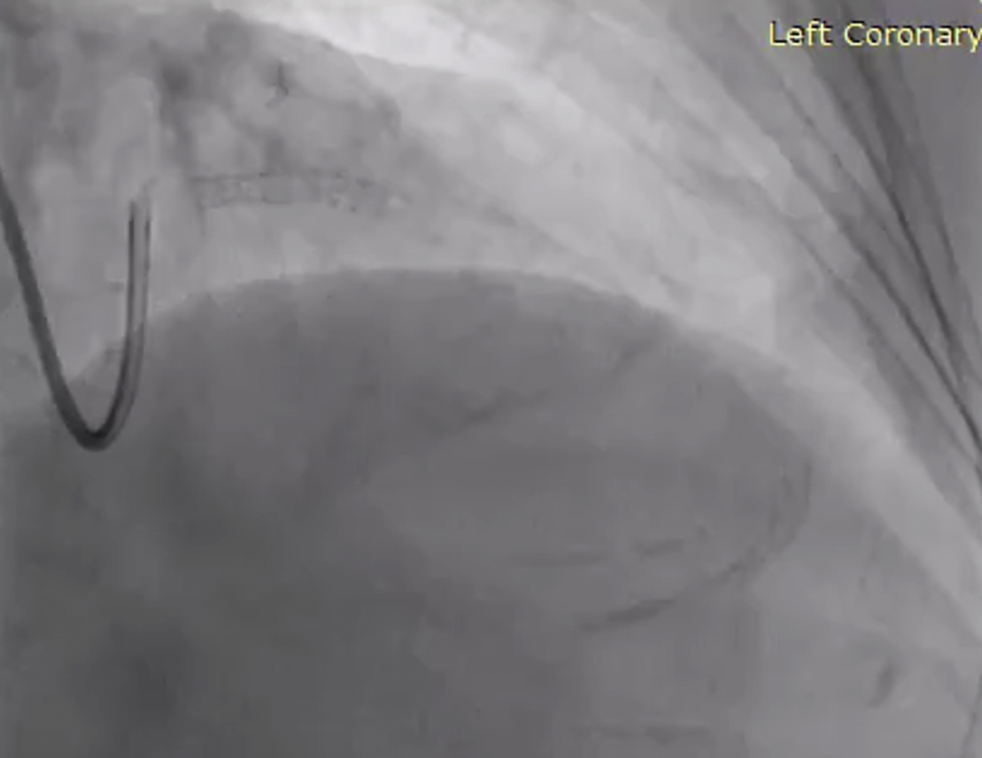
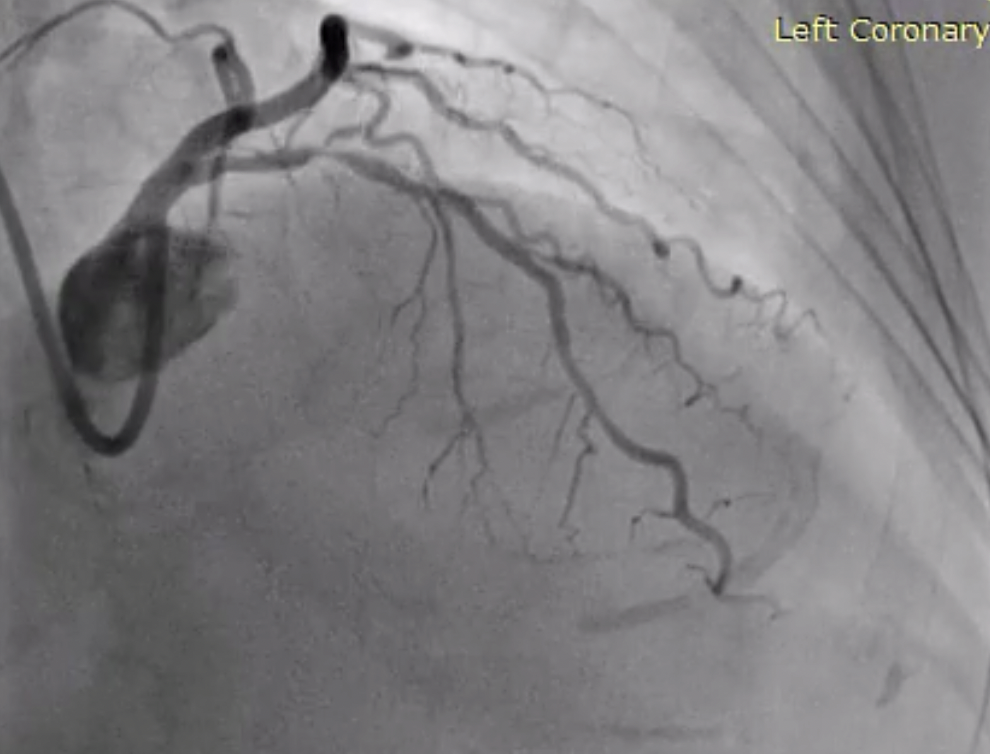
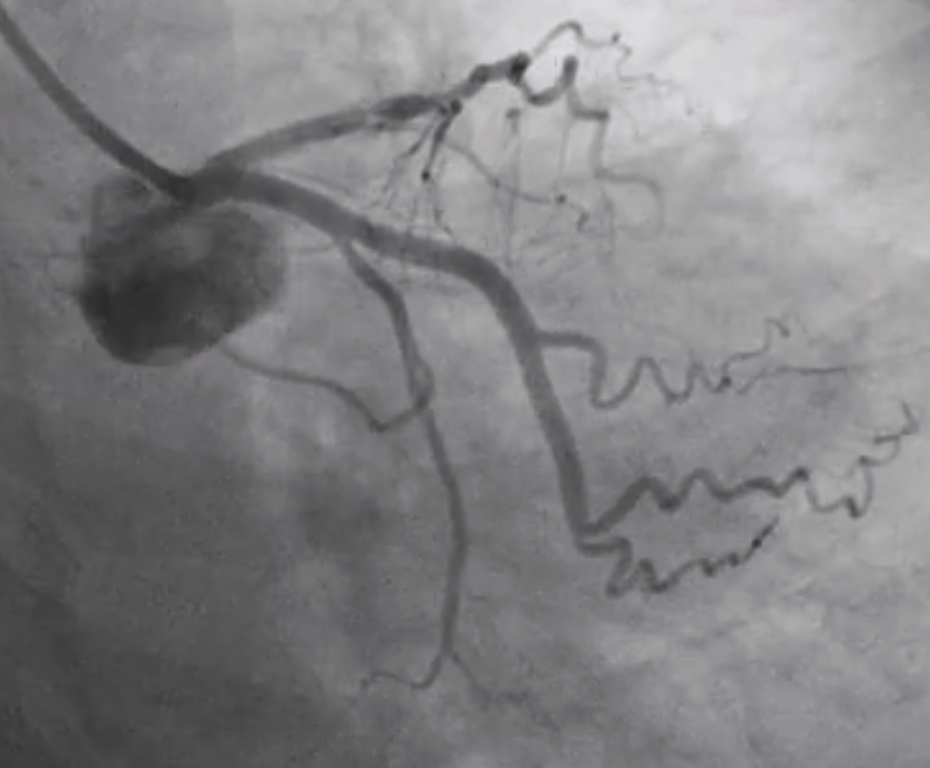
A 77 years female with diabetes, hypertension and post PCI to proximal LAD in 2005 with bare metal stent was presented with stable angina. Her physical examination was unremarkable and LV function was normal. Coronary angiogram showed diffuse Instent restenosis(ISR). In LAD with non-obstructive disease in LCX and RCA. Since she was symptomatic on maximal medical management, PCI to LAD ISR was planned under OCT guidance.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
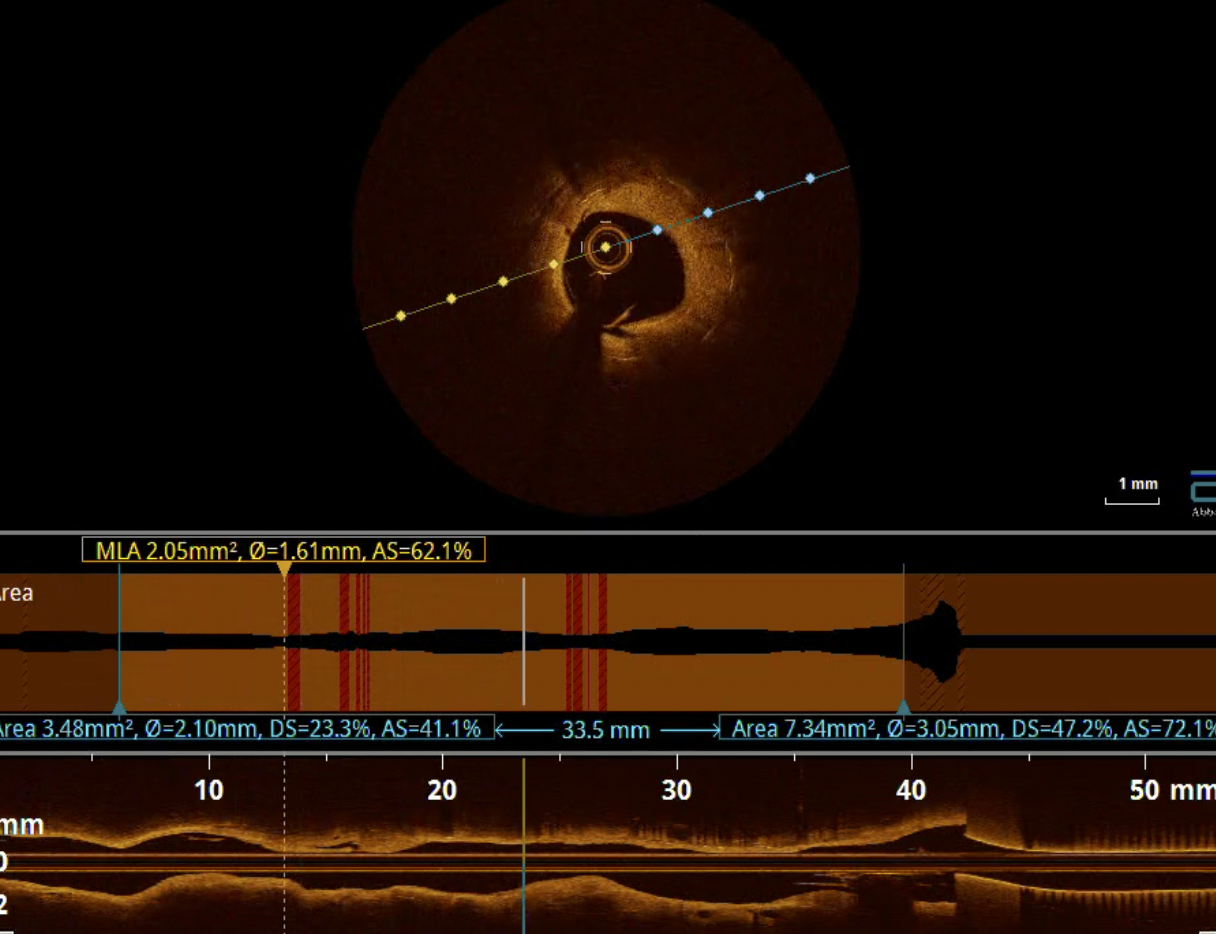
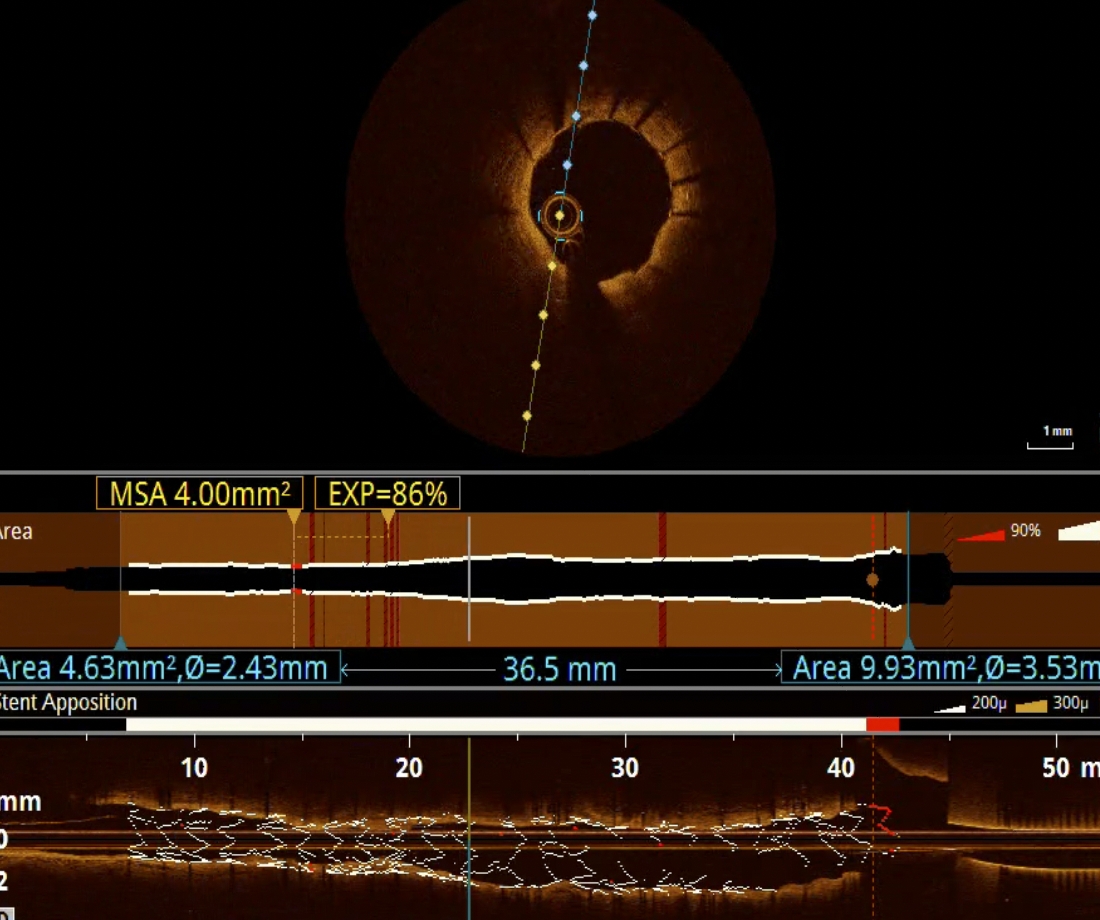
The lesion was pre-dilated with 2.5 mm non compliant balloon to facilitate the passage of OCT catheter. OCT was performed which showed diffuse ISR with neo intimal hyperplasia(NIH). The length of the lesion was 32 mm and reference diameters were 2.5 mm and 3.0 mm at distal and proximal respectively on OCT.
Interventional Management
Procedural Step
As the pre procedural OCT( Dragon fly optis by Abbott cardiovascular) shows thick neo intimal hyperplasia in ISR region, the lesion was prepared with 3 mm Wolverine cutting balloon and further dilated with 3 mm non-compliant balloon at higher pressures. After confirming the expansion of 3 mm balloon in two orthogonal views the lesion was stented with 2.75 x 33 mm everolimus drug eluting Xience stent( by Abbott ) and further optimised with 3 mm non-compliant balloon. Post procedure OCT showed well expanded stent with no edge dissection but with mild un apposition at LAD ostium with was later corrected with 3.5 non-compliant balloon.


Case Summary
Older age, female sex, diabetes and presence of bare metal stent are risk factors for ISR. Intra coronary imaging is necessary to characterise the mechanisms of ISR and to guide management. Optical coherence tomography(OCT) allows for better tissue characterisation of ISR. Diffuse neo intimal hyperplasia pattern of ISR is more in bare metal stents than neo atherosclerosis pattern. Lesion preparation with special balloons like cutting balloon may require in ISR. Repeated DES implantation after proper lesion preparation is the more effective treatment strategy for 1-layer stent