
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-119
Coronary Vasospasm Causing Abrupt Closure of Coronary Artery After Coronary Intervention
By Eran Wen Jun Sim, Cliff Li, Fahim Jafary
Presenter
Cliff Li
Authors
Eran Wen Jun Sim1, Cliff Li1, Fahim Jafary1
Affiliation
Tan Tock Seng Hospital, Singapore1,
View Study Report
TCTAP C-119
Coronary - Complication Management
Coronary Vasospasm Causing Abrupt Closure of Coronary Artery After Coronary Intervention
Eran Wen Jun Sim1, Cliff Li1, Fahim Jafary1
Tan Tock Seng Hospital, Singapore1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
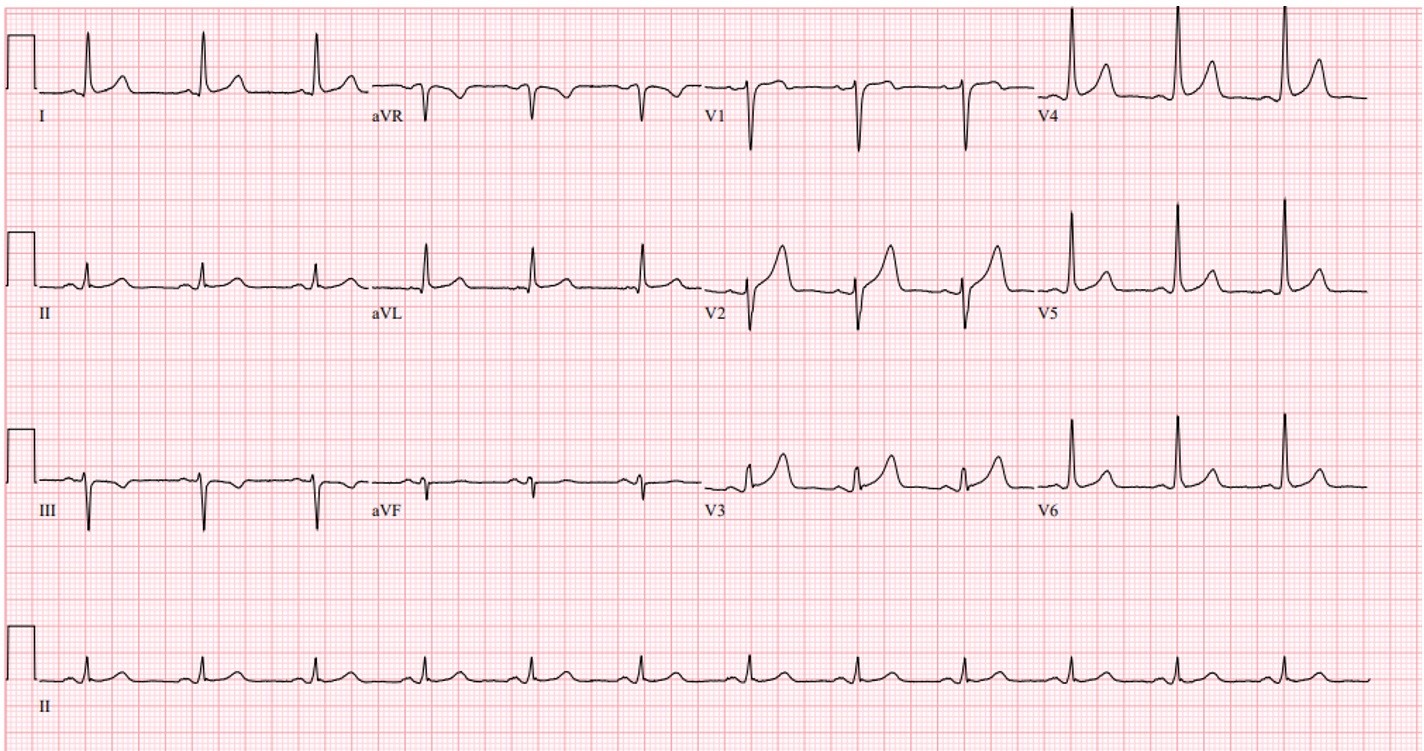
Abrupt closure during coronary intervention is a feared complication whichmay be due to a plethora of reasons not limited to coronary dissection,embolization or coronary artery vasospasm. Our patient was a 62 year oldvocational driver with a significant history of smoking who presented withnon-ST segment elevation myocardial infarction. Initial ECG showed normal sinus rhythm.
Relevant Test Results Prior to Catheterization
A transthoracic echocardiogram show a leftventricular ejection fraction of 45% with regional wall motion abnormalities inthe left anterior descending (LAD) and right coronary artery territories. Hewas brought to our invasive cardiac lab and coronary angiogram was done
Relevant Catheterization Findings
Initial coronary angiogram revealed diffused 60% disease in the ostial andproximal LAD artery, with significant myocardial bridging in the mid LAD. Noculprit infarct related artery was identified. Physiological assessment of the LAD distal to the myocardial bridgingrevealed a fractional flow reserve (FFR) value of 0.7 after 100mcg ofintra-coronary adenosine and the greatest jump during pullback was noted in themid LAD just proximal to the myocardial bridging segment..


Interventional Management
Procedural Step
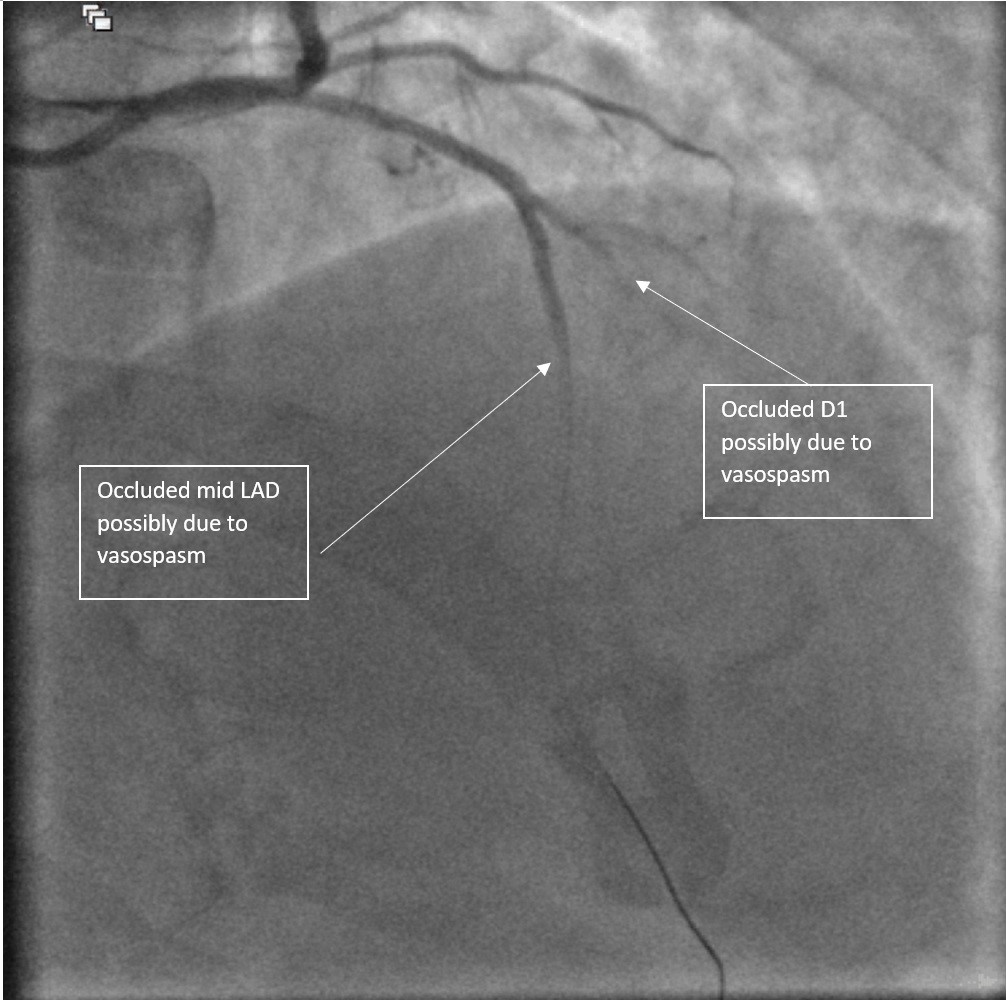
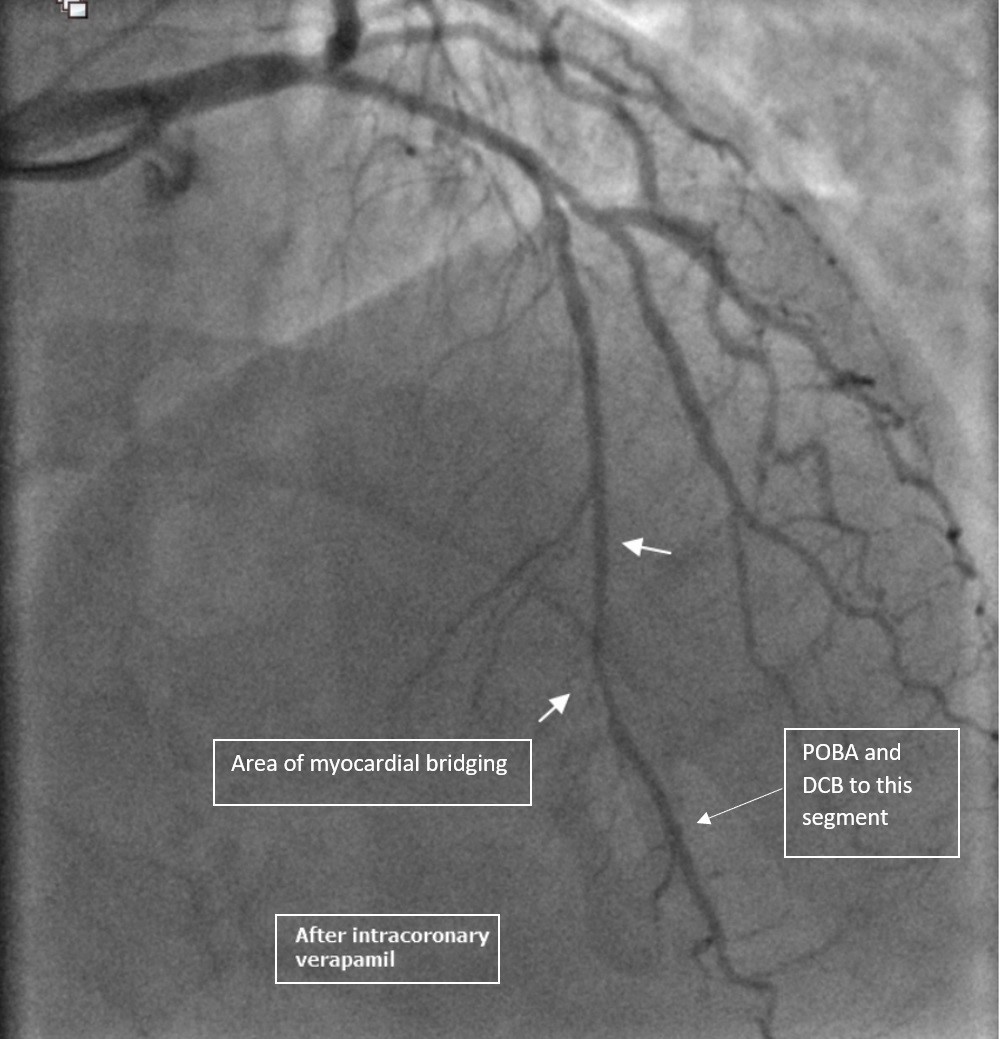
At this juncture, cardiac monitoring revealed ST segmentelevations in the anterior leads and repeat assessment of the LAD revealedocclusion of the mid LAD proximal to the myocardial bridging as well as first diagonalbranch (D1). Intracoronary adenosine and nitroglycerine (GTN) was adminsiteredwith rapid improvement of D1 flow but mid LAD remain occluded. Given the response to intracoronary vasodilators, vasospasmwas a possible etiology. However, due to the persistent occulusion in the midLAD segment, sequential dilation of the mid LAD with a 1.5 X 15mm compliantballoon was performed with achievement of antegrade flow. Additionalintracoronary GTN and nicardipine was administered with resolution of thecoronary spasm. A 2.0 X 20mm drug coated balloon (DCB) was then inflated at themid LAD segment which underwent balloon angioplasty earlier.
Case Summary
Coronary vasospasm is an overlooked etiology of abruptclosure and can even lead to sudden cardiac death because of the dilemmainvolved in the diagnosis. Smoking is one of the factors implicated asrisk factors for the occurrence of coronary vasospasm. Coronary vasospasm tendsto respond well to nitrates and calcium channel blockers and our patient showedsignificant improvement of coronary flow after intra-coronary administration ofnitrogylcerine, nicardipine and verapamil. Early recognition of coronary spasmas a possible etiology for abrupt closure after coronary angiography istherefore extremely important, allowing for early treatment and thus reversal of a potentially fatal disease.