
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-045
The Wave of a Hanging Rock
By Noor Yuhyi Sulaiman, Abdul Ariff, Vekky Sariowan, Huzairi Sani, Shaiful Azmi Yahaya
Presenter
Noor Yuhyi Sulaiman
Authors
Noor Yuhyi Sulaiman1, Abdul Ariff1, Vekky Sariowan2, Huzairi Sani3, Shaiful Azmi Yahaya1
Affiliation
National Heart Institute, Malaysia1, Sam Ratulangi University Manado, Indonesia2, Hospital Pantai Klang, Malaysia3,
View Study Report
TCTAP C-045
Coronary - Complex PCI - Calcified Lesion
The Wave of a Hanging Rock
Noor Yuhyi Sulaiman1, Abdul Ariff1, Vekky Sariowan2, Huzairi Sani3, Shaiful Azmi Yahaya1
National Heart Institute, Malaysia1, Sam Ratulangi University Manado, Indonesia2, Hospital Pantai Klang, Malaysia3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
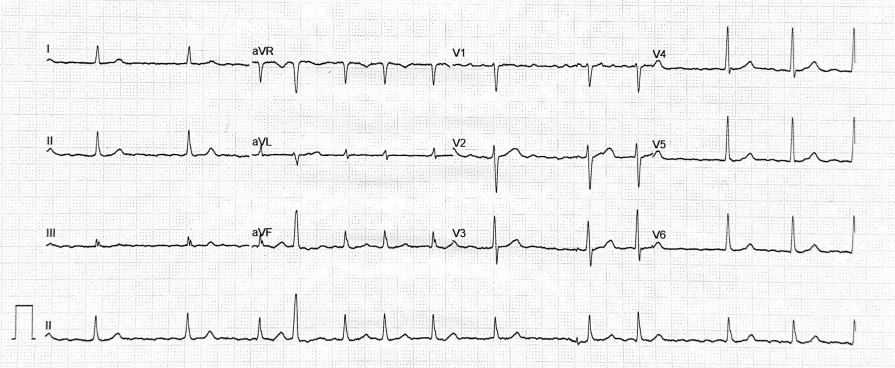
60-year-old gentleman with a background history of Hypertension, Atrial Fibrillation (AF), Ischemic heart disease (IHD)Presented with chest pain, associated with palpitation, and diaphoresis. Baseline CCS II-III, NYHA II. On arrival he had a HR of 150bpms, irregular, lungs was clear and BP 164/114. Cardiac monitor showed AF, which subsequently cardioverted to sinus rhythm. ECG Sinus rhythm, no significant ST-T changes. Echocardiogram during admission LVEF 42%, No regional wall abnormalities
Relevant Test Results Prior to Catheterization
| Renal Profile | |
| Na | 138 |
| K | 3.9 |
| Urea | 2.4 |
| Creat | 86 |
| Lipid Studies | |
| TC | 2.6 |
| HDL | 1.3 |
| LDL | 0.8 |
| TG | 1.2 |
| HbA1C | 5.8 |
| FBC | |
| Hb | 14.5 |
| Hct | 32.8 |
| Wbc | 11.5 |
| Platelet | 258 |
| | |


Relevant Catheterization Findings
Coronary Angiogram
- Left Main Stem : Severe stenosis distal Left Main Stem , calcified
- Left Anterior Descending : Moderate stenosis proximal Left Anterior Descending , calcified
- Left Circumflex : Mild stenosis ostial Left Circumflex , moderate stenosis mid Left Circumflex
- Right Coronary Artery : Normal
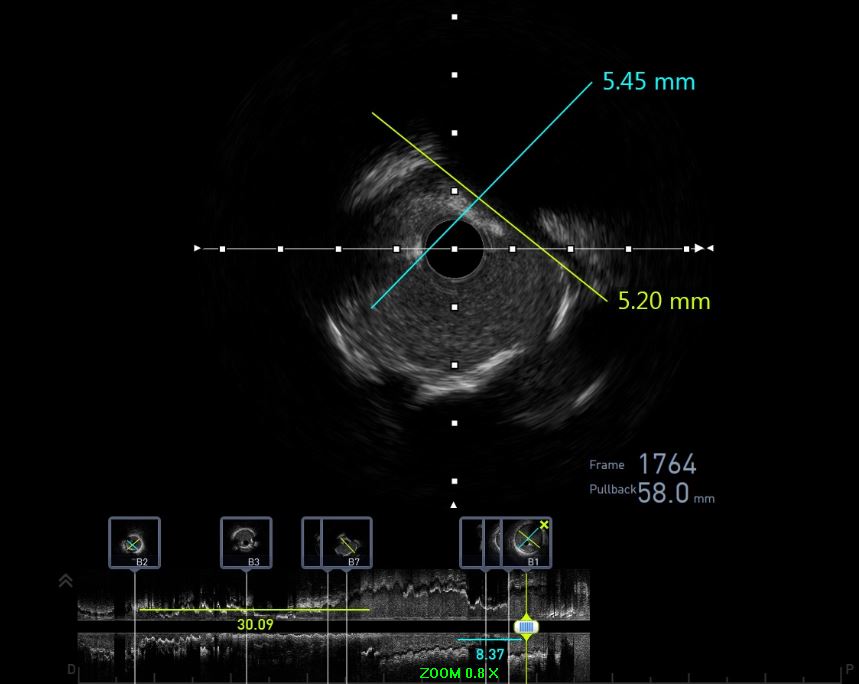
IVUS Pre PCI
LMS: Calcium nodule, Vessel size 5.2mmLAD: Ostial LAD 270 lesion pLAD 4.0mmLCX: Ostial LCX MLA 6.5mm2 plaque burden 50%
Interventional Management
Procedural Step
LMS: LAD 2 calcium nodule @ LMS ostial LAD LM 5.0mm pLAD 4.0mmLCX Ostial LCX MLA 6.5 plaque burden 50%
2 wires inserted Run-through floppy wired down to LAD Sion blue wired to protect LCX
PCI to LMPredilated LMS:Wedge NC 2.5/15mm @ 22 atms Scoreflex 3.5/15 @ 22 atms Wolverin 4.0 /10@ 16atms NC Accuforce 4.0/12@ 22atms Was not able to crack Calcium nodule
IVL with shockwave C2 4.0/12mm dLMS Ostial LAD for 80 pulses NC Accuforce 4.0/12mm @ 22 atms Finally able to crack the calcium
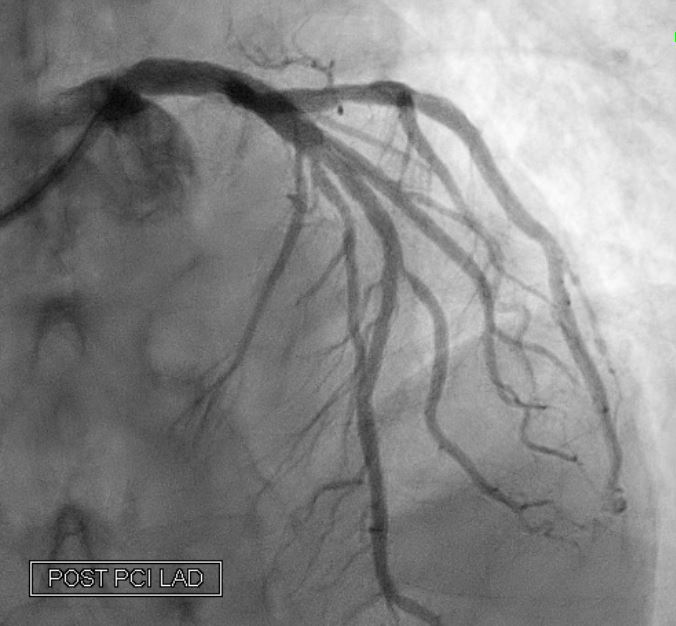
Stented with Megatron 4.0x20mm 11atms@8-12atms post dilated NC Accuforce 4.0X12mm 8-24@ 9-12sec
Kissing Balloon was done LAD Accuforce NC 4.0/12mm LAD 12 atms @ 9-15secLCX NC Sapphire NC 3.0/8mm LCX 12 atms @ 10sec
Final POT with Accuforce 5.0/8mm 12atms @ 12sec
Relook IVUS LAD stent well opposed No stent edge dissection No hematoma


2 wires inserted Run-through floppy wired down to LAD Sion blue wired to protect LCX
PCI to LMPredilated LMS:Wedge NC 2.5/15mm @ 22 atms Scoreflex 3.5/15 @ 22 atms Wolverin 4.0 /10@ 16atms NC Accuforce 4.0/12@ 22atms Was not able to crack Calcium nodule
IVL with shockwave C2 4.0/12mm dLMS Ostial LAD for 80 pulses NC Accuforce 4.0/12mm @ 22 atms Finally able to crack the calcium
Stented with Megatron 4.0x20mm 11atms@8-12atms post dilated NC Accuforce 4.0X12mm 8-24@ 9-12sec
Kissing Balloon was done LAD Accuforce NC 4.0/12mm LAD 12 atms @ 9-15secLCX NC Sapphire NC 3.0/8mm LCX 12 atms @ 10sec
Final POT with Accuforce 5.0/8mm 12atms @ 12sec
Relook IVUS LAD stent well opposed No stent edge dissection No hematoma
Case Summary
The presence of calcification in coronary bifurcation lesions increases the complexity of these already challenging PCI procedures. Hence Intravascular imaging should be used to guide each step of complex PCI (at baseline, after lesion preparation, and post-stent implantation), informing decisions regarding the most appropriate technique for calcium modification and confirming optimal stent expansion. The failure to crack the calcium despite using a scoring balloon / wolverine / and a high pressure NC balloon, shows the benefit IVL in cracking severely calcified lesions and delivering good results without increasing complications.