
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-096
Lifeline Hanging by a Short Thread-Like Left Main
By Huzairi Sani, Wei Liang Lee, Yee Sin Tey, Shaiful Azmi Yahaya
Presenter
Huzairi Sani
Authors
Huzairi Sani1, Wei Liang Lee2, Yee Sin Tey2, Shaiful Azmi Yahaya2
Affiliation
Hospital Pantai Klang, Malaysia1, National Heart Institute, Malaysia2,
View Study Report
TCTAP C-096
Coronary - Complex PCI - Left main
Lifeline Hanging by a Short Thread-Like Left Main
Huzairi Sani1, Wei Liang Lee2, Yee Sin Tey2, Shaiful Azmi Yahaya2
Hospital Pantai Klang, Malaysia1, National Heart Institute, Malaysia2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
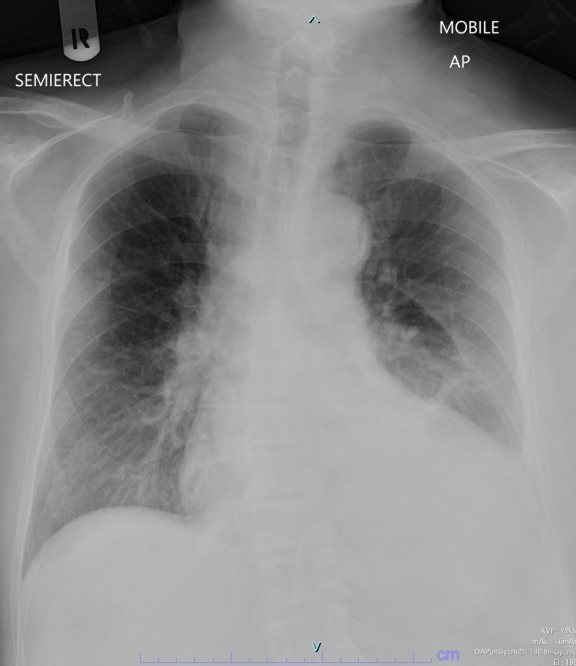
A 73-year-old gentleman with background medical history of Hypertension, Dyslipidemia, End stage renal disease and a recent NSTEMI presented with typical angina during hemodialysis. His recent NSTEMI reported as triple vessel disease with left main involvement which was planned for elective Percutaneous Coronary Intervention (PCI).

Relevant Test Results Prior to Catheterization
ECHO: Moderately reduced left ventricular function. Biplane EF = 36%. Hypokinetic areas seen at rest. No significant valvular disease.
Haemoglobin: 9.7 g/dl , White blood cell: 7.3 x10^9/l , Platelet count: 201 x10^9/lUrea: 8.8 mmol/l , Creatinine: 375 umol/lTotal cholesterol: 2.7 mmol/L Triglycerides: 1.0 mmol/L HDL-cholesterol: 0.7 mmol/L LDL-cholesterol: 1.5 mmol/LGlucose: 5.3 mmol/L

Haemoglobin: 9.7 g/dl , White blood cell: 7.3 x10^9/l , Platelet count: 201 x10^9/lUrea: 8.8 mmol/l , Creatinine: 375 umol/lTotal cholesterol: 2.7 mmol/L Triglycerides: 1.0 mmol/L HDL-cholesterol: 0.7 mmol/L LDL-cholesterol: 1.5 mmol/LGlucose: 5.3 mmol/L
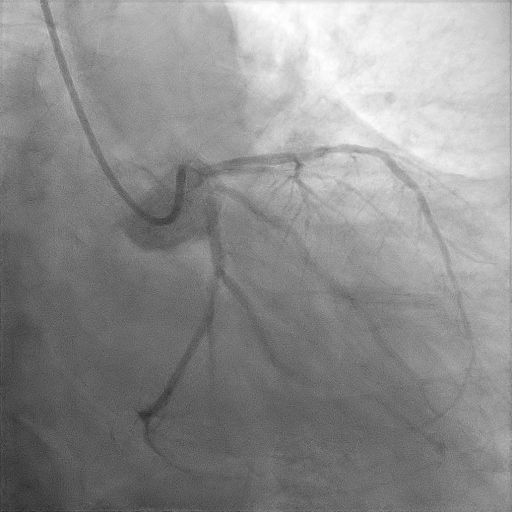
Relevant Catheterization Findings
Access: Right femoral artery IABP inserted via left femoral artery EBU 3.5 7Fr guiding catheterRunthrough floppy wire to left circumflex and SION blue wire to LAD. IVUS run from LAD - Mid LAD 3.84 mm2 with 68% plaque burden. Ostial LAD 5.56mm2 and 65% plaque burden. Diffusely disease with fibrocalcific plaques and areas of 270 to 360 degrees calcium. Very short left main. IVUS run from LCx - Calcified 270-360 degree calcium. Ostial LCx 3.1 mm2.
Interventional Management
Procedural Step
LAD - ROTA 1.5mm burr size for long calcified lesions with superficial calcium.



Assess plaque modification effect - Calcium fractures
Scoring balloon to increase MLA and increase fractures to assure stent expansion is optimal.
2-stent strategy, DES 3.5 x 28 mm and 4.0 x 20 mm deployed from LM - mid LAD.
Unable to ROTA the left circumflex due to short left main.
Adequate lesion preparation with cutting balloon then proceeded 2-stent strategy, DES 3.5 x 16 mm (Mini-crush technique).
Followed by kissing balloon inflation and POT.
Case Summary
PCI of the calcified short left main coronary bifurcation lesion is possible with the advancement of technique and technology. Vessel preparation and plaque modification are extremely crucial before a stepwise 2-stent technique decision.