
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-083
Solving Recalcitrant Instent Restenosis With Combined Laser Atherectomy and Shockwave Intravascular Lithotripsy
By Sakolwat Montrivade
Presenter
Sakolwat Montrivade
Authors
Sakolwat Montrivade1
Affiliation
Police General Hospital, Thailand1,
View Study Report
TCTAP C-083
Coronary - Complex PCI - In-Stent Restenosis
Solving Recalcitrant Instent Restenosis With Combined Laser Atherectomy and Shockwave Intravascular Lithotripsy
Sakolwat Montrivade1
Police General Hospital, Thailand1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 68-year-old man with past medical history of hypertension, atrial fibrillation and chronic coronary disease presented with worsening angina for 2 months. He had prior PCI of OM and RCA with a total of 5 stents in 2006. There was recurrent angina in 2021 that was treated with a 3.5 x 15 mm stent placed at the RCA ostium. Nuclear stress test revealed perfusion defect in the inferior segments together with hypokinesis in this area consistent with myocardial infarction.

Relevant Test Results Prior to Catheterization
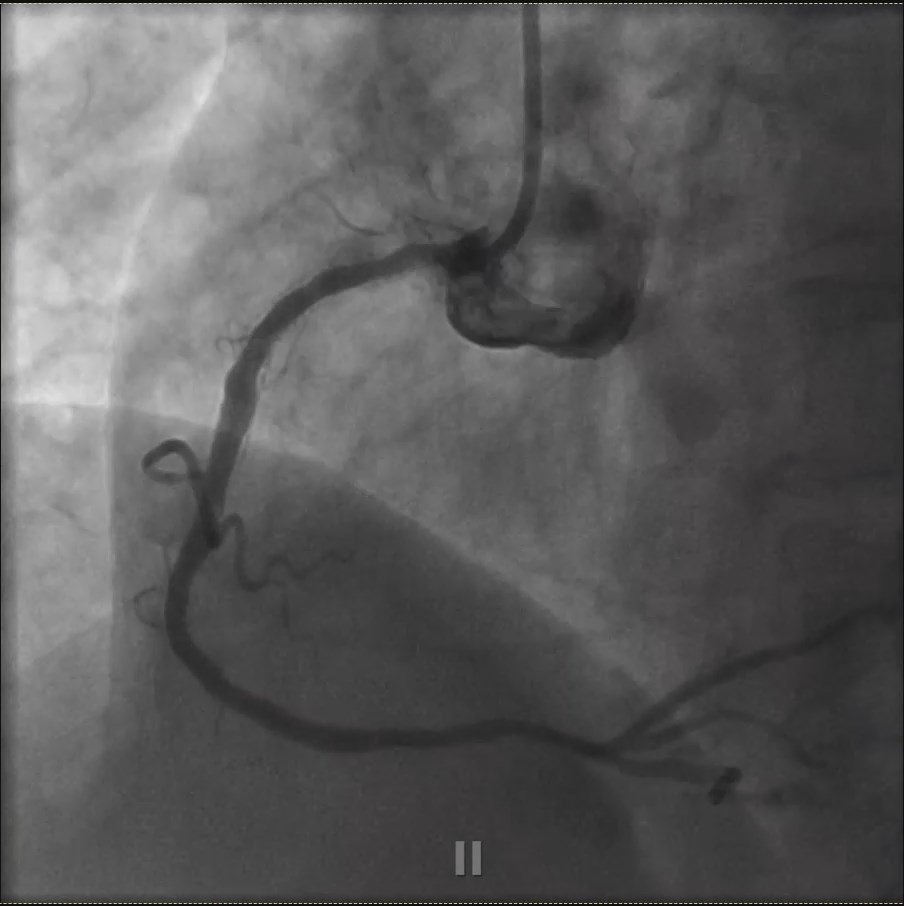
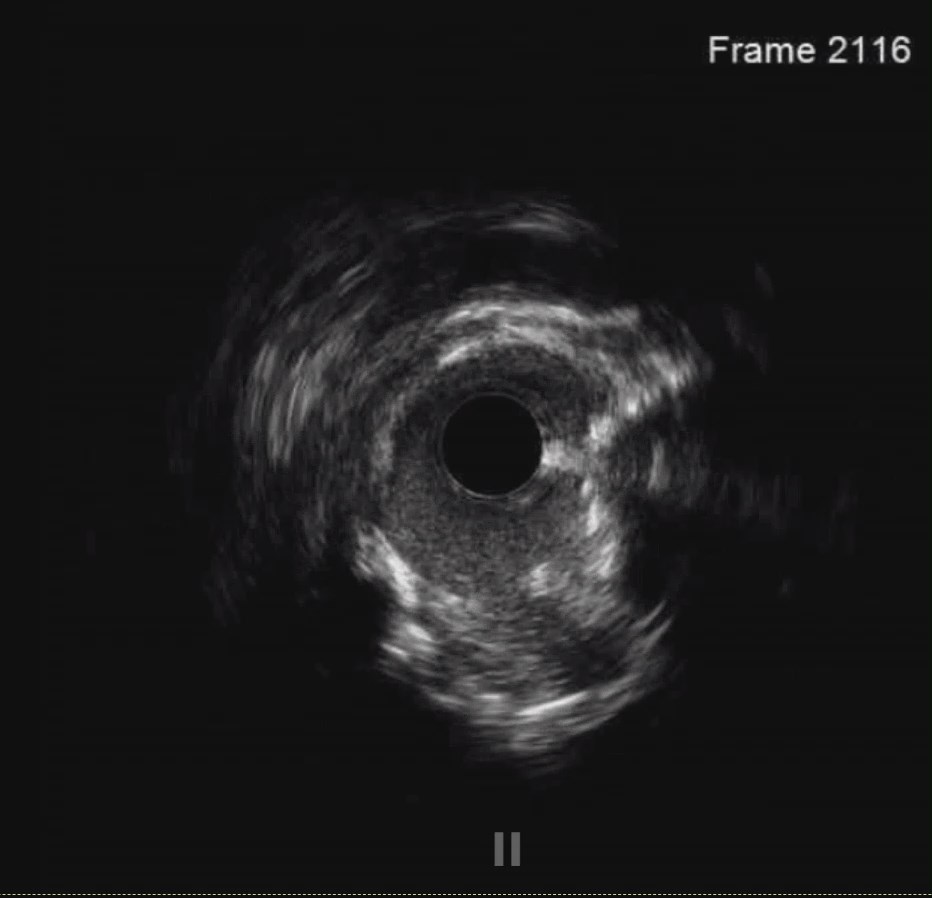
We brought the patient for coronary angiography and found 90% instent restenosis of the ostial RCA which we treated with POBA using NC 4.0 mm balloon inflated at high pressure. IVUS revealed underexpanded stent on heavily calcified RCA ostium. There was also a borderline 30-40% stenosis of the left main ostium that we used IVUS to measure luminal area and found acceptable MLA of 8.5 mm2.
Relevant Catheterization Findings
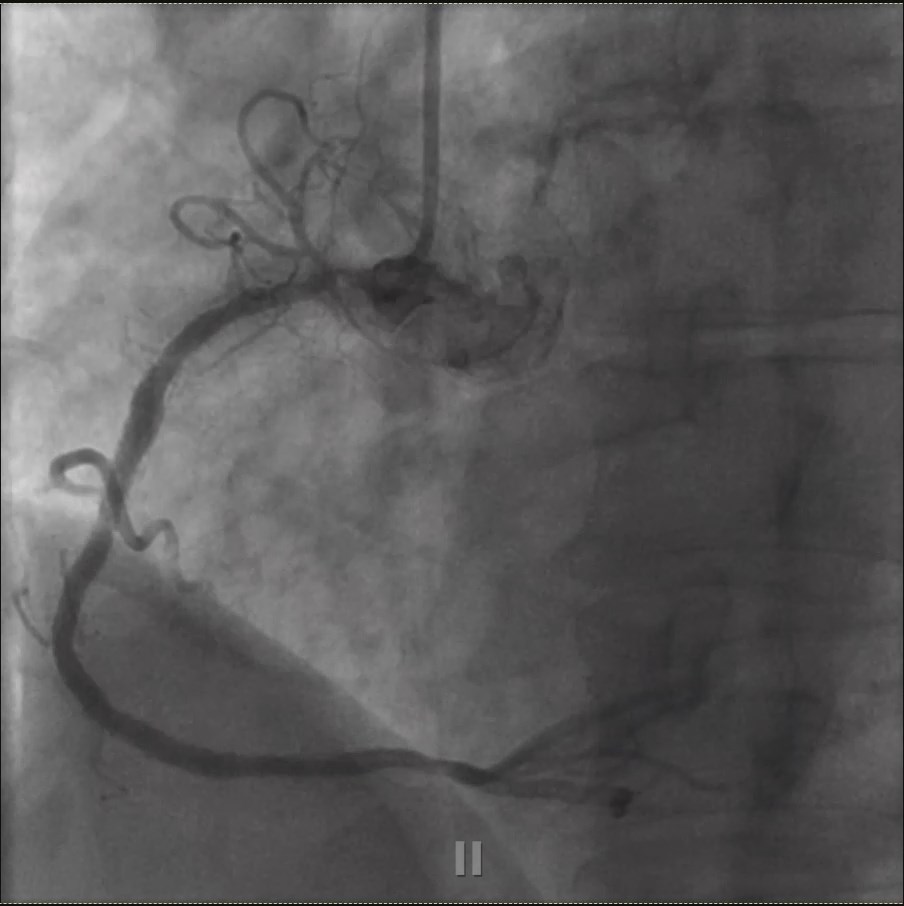
Unfortunately, the patient developed recurrent angina after 6 weeks of POBA. We then brought the patient for repeat coronary angiography which revealed 95% recurrent ISR of the RCA ostium and 70% stenosis of mid RCA. LM had unchanged 30-40% ostial stenosis.
Interventional Management
Procedural Step
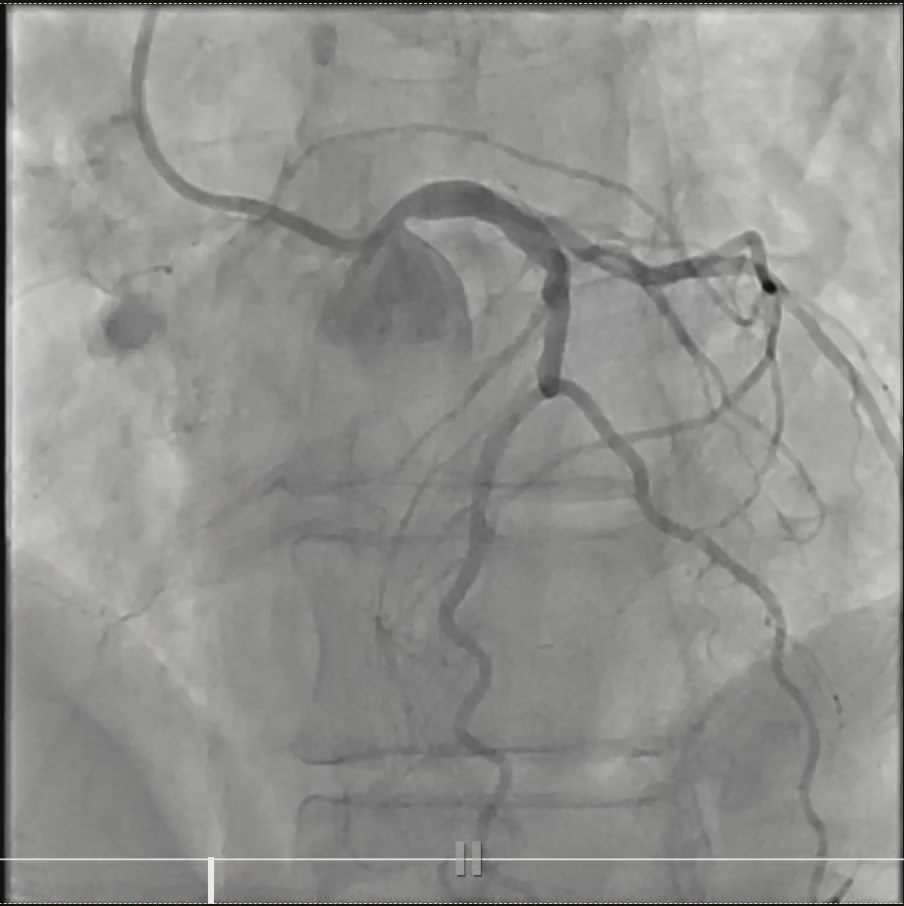
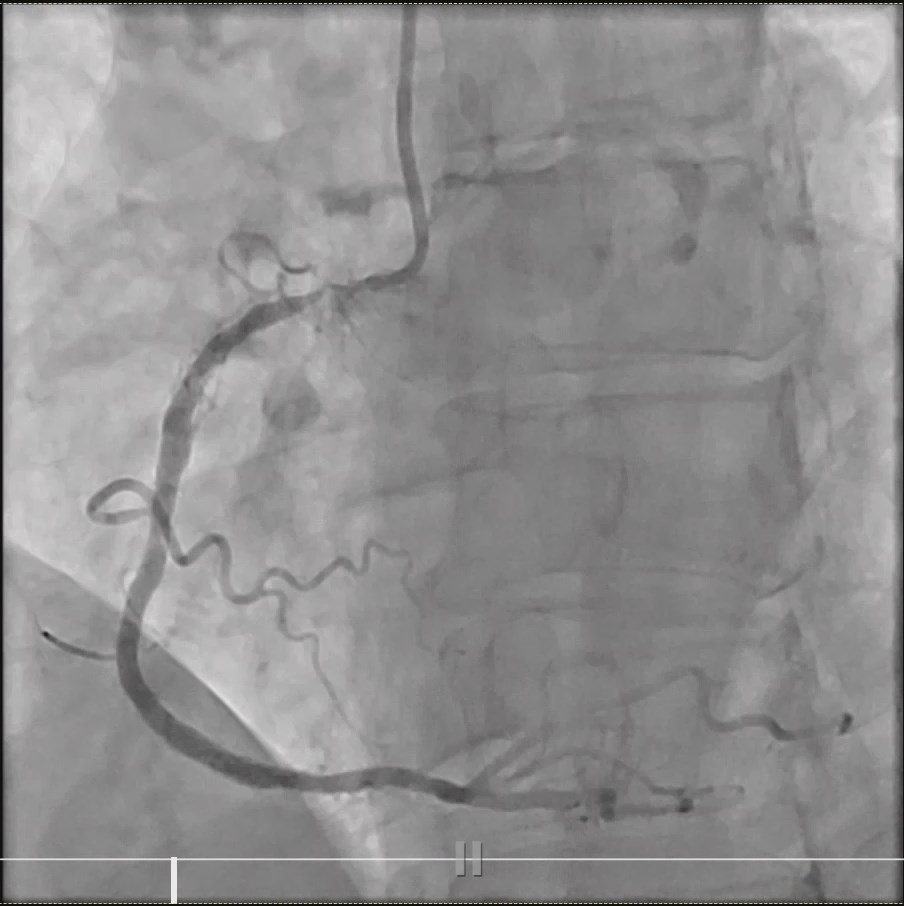
We engaged RCA with AL1 guiding catheter and passed a workhorse wire to distal RCA. We then performed laser atherectomy using 1.7 mm catheter with maximum fluency and contrast injection for 33 seconds. IVUS revealed severely under-expanded stent with a diameter of less than 3.0 mm in a very large vessel with deep circumferential calcification. We then performed Shockwave intravascular lithotripsy using IVL 4.0 x 12 mm inflated at 6 atm for 80 pulses. The lesion was further dilated with NC 4.0 mm and NC 5.0 mm balloons at 20 atm with great balloon expansion. Stent enhancement image (clearstent) found a gap between stents and evidence of stent struts fractures in the ostial RCA stent, despite very good expansion on IVUS. Ultimately, we stented proximal RCA with Resolute Onyx Frontier 5.0 x 22 mm at 14 atm up to the ostium and post-dilated the stent with NC 5.0 mm balloon. Mid RCA was also stented with Resolute Onyx Frontier 4.0 x 22 mm with good result. . Final IVUS revealed fully expanded and well-apposed all stents, proximal RCA MLA was large with diameter of >5 mm.


Case Summary
In recalcitrant ISR lesions, intravascular imaging play a crucial role of determining PCI strategy. In this case, we found underexpanded stent with underneath deep circumferential calcification. These findings suggest the use of aggressive lesion preparation. Laser atherectomy is an excellent tool to ablate the underexpanded stent and shockwave intravascular lithotripsy is the best option to solve deep calcification under the prior stent. Lastly, enhanced stent imaging system provides better understanding of the prior stent after laser ablation and shockwave, revealing stent gap and fractures that prompt restenting over the ISR lesion covering the stent gap and stent factures.