
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-174
A Case of IVUS-Guided LM Ambiguous Lesion Treatment
By Yingqian Zhang, Changfu Liu, Yun-Dai Chen
Presenter
Yingqian Zhang
Authors
Yingqian Zhang1, Changfu Liu1, Yun-Dai Chen1
Affiliation
Chinese People's Liberation Army General Hospital, China1,
View Study Report
TCTAP C-174
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
A Case of IVUS-Guided LM Ambiguous Lesion Treatment
Yingqian Zhang1, Changfu Liu1, Yun-Dai Chen1
Chinese People's Liberation Army General Hospital, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 82-year-old manpresented to Chinese PLA General Hospital, Beijing, China, with chest pain onminimal exertion. He suffered from chest pain and had 1 stent inplantation inLAD and 1 stent in LCX in 2013. In 2020, he suffered from STEMI, and had 1stent inplantation in RCA. On admission, his blood pressure was 125/80 mm Hg,HR was 58 beats/min. Heart and lung auscultation findings were unremarkable.ECGshowed pathological Q wave in leads II, III and aVF.Theechocardiogram showed EF45%,RWMV.
Relevant Test Results Prior to Catheterization
Hisinitial peak troponin level was 0.024 ng/ml (normal value <0.01ng/ml). Hisfast glucose was 8.11mmol/L(normal value <6.1mmol/L). The nt-proBNP was186.8pg/ml at administration(normal value <150pg/ml). The LDL-c was0.73mmol/L. HAb1c was 9.9% at administration(normal value <6.0%).
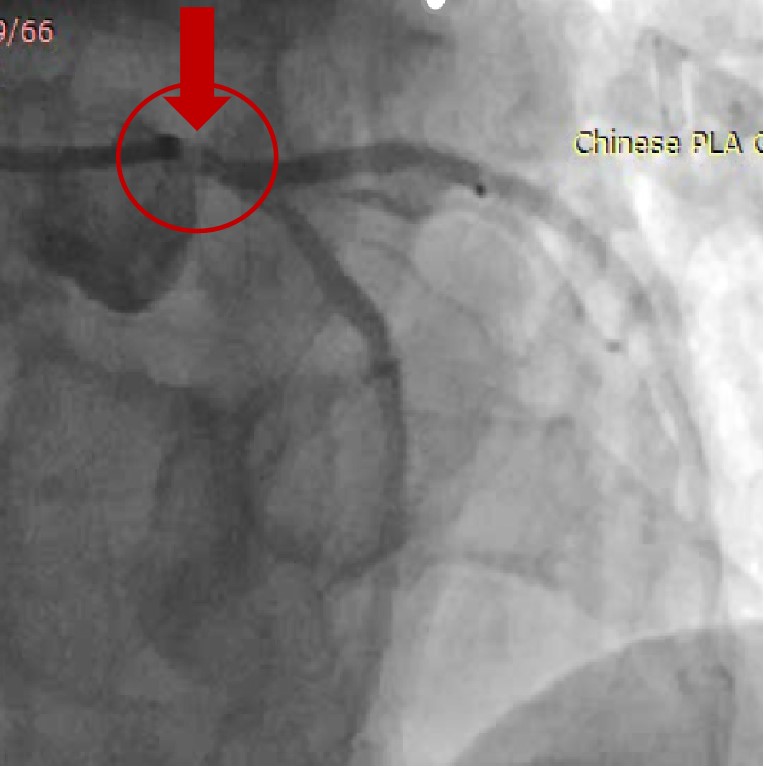
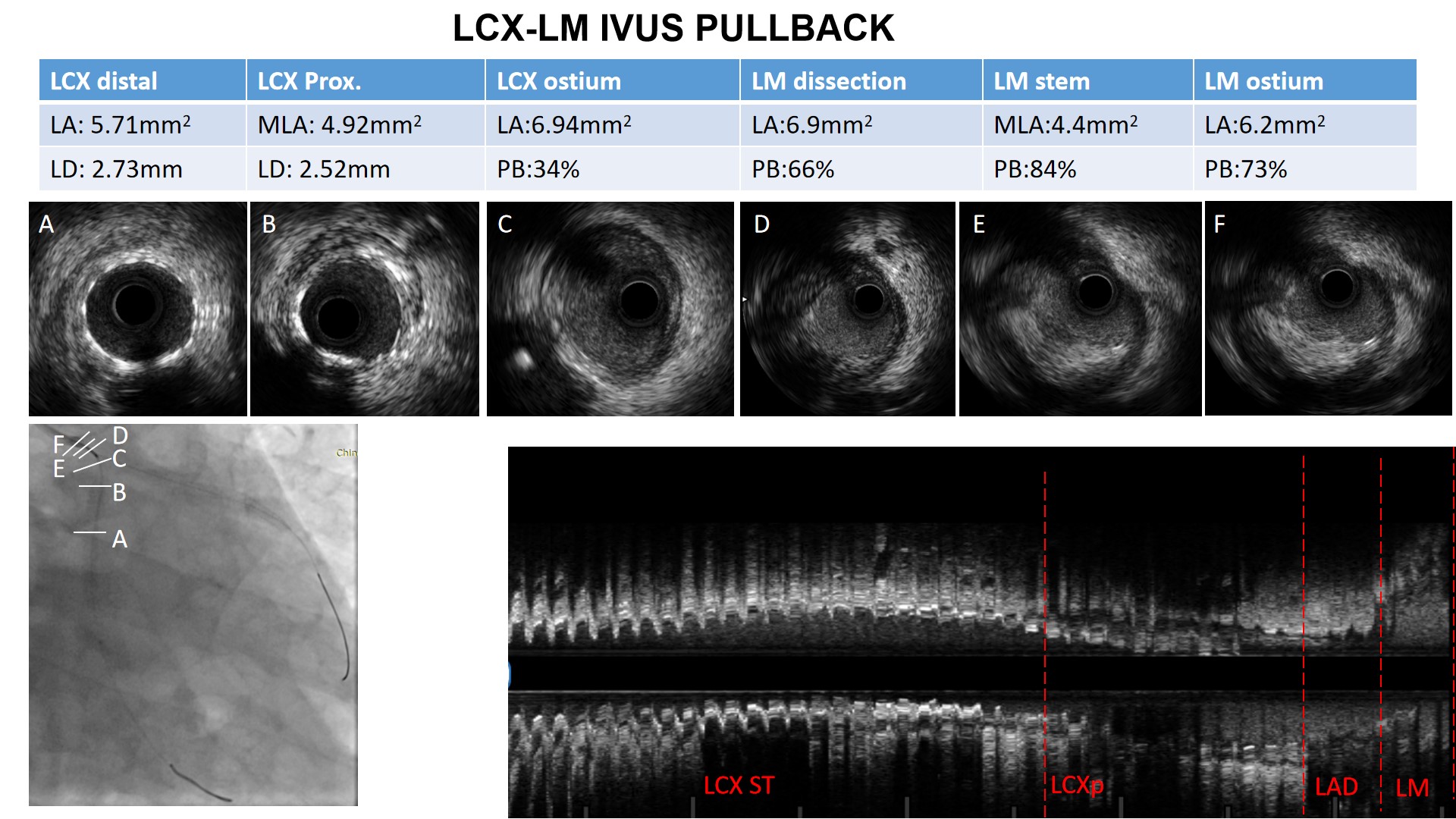
Relevant Catheterization Findings
Angiographyrevealed LM ambiguous lesion. There was no in-stent restenosis in LAD, LCX andRCA. IVUS revealed a dissection flap in the the end of LM, with the lumen areaof 6.9mm2, and 66% plaque burden. There was sever stenosis in the stem of LM,with the minimal lumen area of 4.4mm2, and 84% plaque burden. The lumen area ofLM ostium is 6.2mm2, and 73% plaque burden. The lumen area of LAD ostium is7.4mm2. The lumen area of LCX ostium is 6.94mm2.
Interventional Management
Procedural Step
Thepatient had LM sever stenosis and dissection. The LM bifurcation lesion was Medina1,1,0. We discussed and decided to explore provisional strategy in LAD-LM. Thereafter,the patient underwent coronary artery angioplasty to the area of dissection.Scoreflex balloon 2.5×20mmwere dilated at 10 atmospheres (atm) across the lesion in the LAD-LM. A PromusPremier 3.5x28 mm stent was deployed at 12 atm. Post-dilation with anon-compliant 3.5×14 mmballoon (Quantum balloon, Boston Scientific Co., Natick, MA) at 16-18 atmachieved full expansion of balloon. Post-dilation with a non-compliant 4.0×8mm balloon(Quantum balloon, Boston Scientific Co., Natick, MA) at 12 atm achievedproximal optimisation (POT). Post-stent IVUS showed good result with no furtherresidual dissection detected and good stent wall opposition and expansion. IVUSrevealed the minimal stent area of proximal LAD is 8.9mm2, with the meandiameter of 3.3 mm. The area of LAD ostium is 7.4 mm2. The minimal stent areain LM is 10.56 mm2. IVUS pullback from LCX to LM showed that the minimal lumenarea of LCX is 6.78 mm2. The area of LCX ostium is 6.6 mm2, with plaque burden33%. A satisfactory result was documented by angiogram and IVUS imaging,respectively. The patient discharge 2 days later on aspirin and clopidogrel.

Case Summary
The LM ambiguous lesions should have intra-coronary imaging toget precise diagnosis. Considering the possibility of dissection, we chose IVUS over OCT. IVUS could identify thrombosis, dissection, calcification,the minimal lumen area, and plaque burden. In the IVUS image of this patient, dissection and severe stenosis with large plaque burden in LM could be detected. Wehighly suspect the occurrence of iatrogenic dissection. Intracoronarystenting of the LAD and LCX can be accomplished using various bifurcationstenting techniques. In this case there was no significant atherosclerosislesion in LCX ostium, thus we choose provisional strategy.