
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-144
AWMI With Ostial LAD Occlusion - A New Thought
By Balakrishna Pai, Musna Jamal
Presenter
MUSNA JAMAL
Authors
Balakrishna Pai1, Musna Jamal2
Affiliation
Adan Hospital, Kuwait1, St Mary's Hospital Thodupuzha, India2,
View Study Report
TCTAP C-144
Coronary - DES/BRS/DCB
AWMI With Ostial LAD Occlusion - A New Thought
Balakrishna Pai1, Musna Jamal2
Adan Hospital, Kuwait1, St Mary's Hospital Thodupuzha, India2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
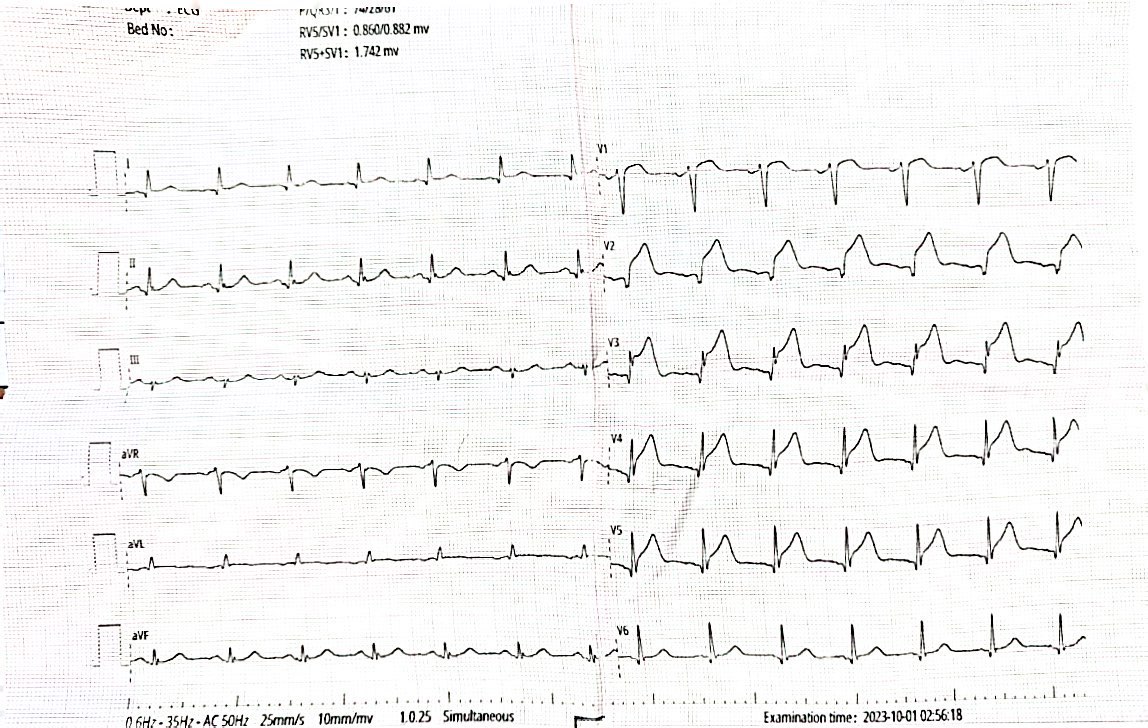
A 34-year-old expatriate, whose residency permit had expired, was rushed to the emergency department after experiencing acute chest pain for three hours. He was a smoker but had no other risk factors. His ECG revealed an acute anterior wall myocardial infarction. He was in Killip's Class 1 and was hemodynamically stable. He was immediately taken for primary PCI.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
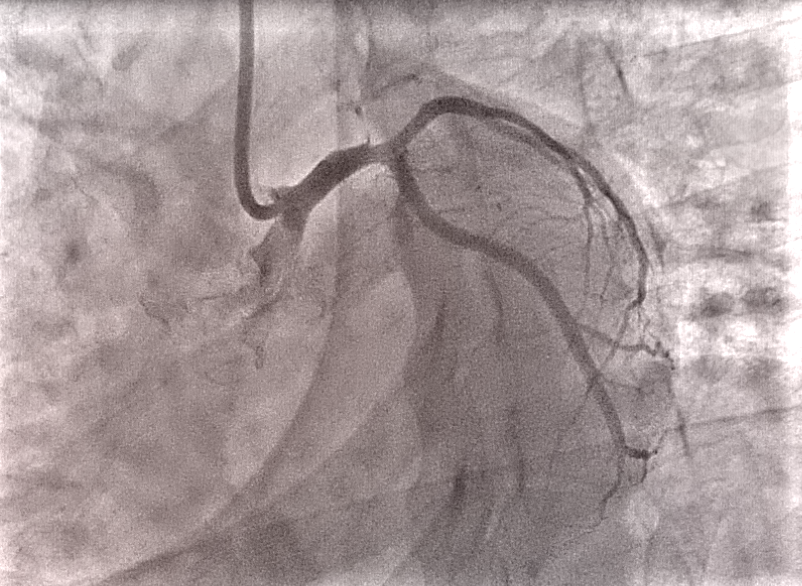
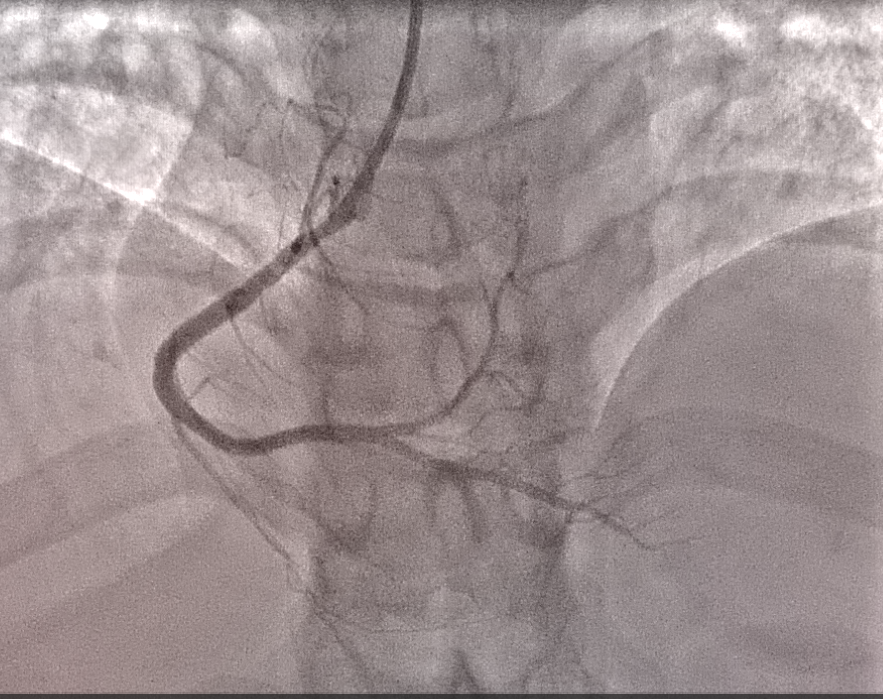
Coronary angiogram was done through the right radial artery using 6F XB 3.5 catheter. Left coronary injection showed occluded LAD from the ostium with minor plaque extension to the left main and ramus intermedius, while the left circumflex ostium was free of stenosis. The Right coronary was normal. The patient needed stenting from the left main to LAD, but due to concerns about the continuation of long-term antiplatelet therapy because of expired residency

Interventional Management
Procedural Step
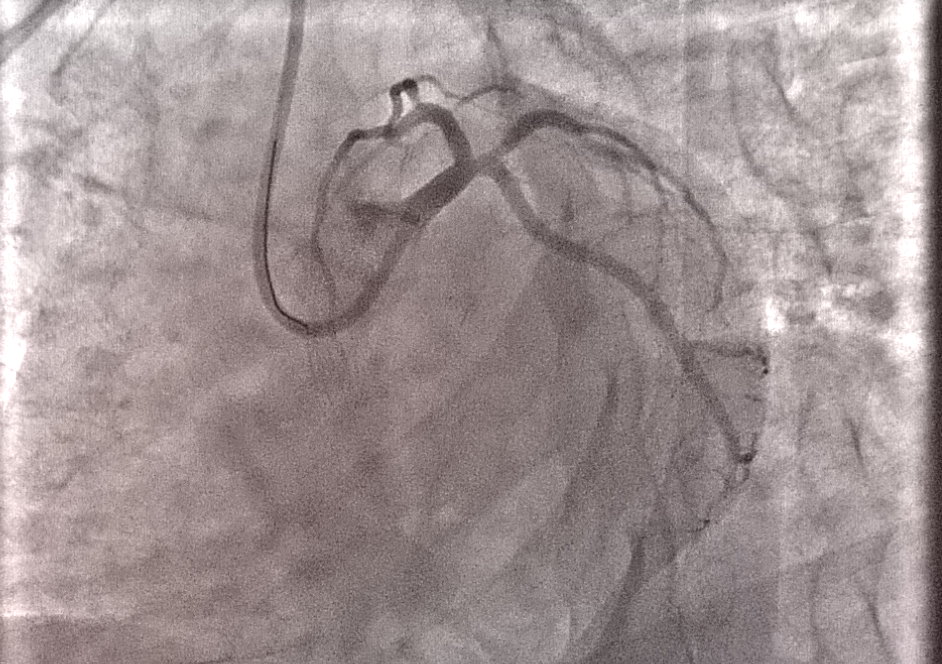
The Runthrough guidewire was used to wire the Left Main coronary to LAD, and the LAD ostium was dilated using a 2.5mmx15mm semi-compliant balloon. The pre-dialation opened the LAD without any dissection or thrombus. Subsequently, a 3mmx 6mm wolverine cutting balloon was used at 16 atm to further dilate the LAD ostium. LAD was opened well with no dissection or slow flow. Therefore drug-eluting balloon dilation (DEB) was done from the distal left main to LAD with 3.5x 20mm MagicTouch SCB (sirolimus-coated drug balloon) at 8 atm for 90 minutes. A good final result was obtained. The patient was kept on tirofiban infusion for 24 hours and was given dual antiplatelets (aspirin, clopidogrel) and high-intensity statin. The patient's echo showed a hypokinetic septum and anterior wall with an ejection fraction of 40%. After three days, the patient was discharged and is currently on six-months follow-up. He is stable and asymptomatic at present.


Case Summary
The use of drug balloons to treat native vessel disease is a new approach, but there isn't enough information about its effectiveness in patients with acute myocardial infarction. The idea is to treat native ostial lesions by combining cutting balloon dilation with a drug-coated balloon (DCB/DEB) to deliver the drug to prevent barotrauma-induced vessel restenosis. The advantage of cutting balloon is that it reduces vessel stretch and injury by scoring the vessel longitudinally, rather than causing an uncontrolled disruption of the plaque. This approach helps to avoid future stent-related events, but it is relatively new and requires further evidence to support its effectiveness.
|
Mohammad Shafiqur Rahman Patwary (NATIONAL INSTITUTE OF CARDIOVASCULAR DISEASES) Apr 25, 2024
|
|
| Nice case | |