
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-044
A Severe Calcified Lasting Artery Case: Percutaneous Coronary Intervention With Rotational Atherectomy
By Trung Minh Tran, Huynh Trung Cang
Presenter
Trung Minh Tran
Authors
Trung Minh Tran1, Huynh Trung Cang1
Affiliation
Kien Giang General Hospital, Vietnam1,
View Study Report
TCTAP C-044
Coronary - Complex PCI - Calcified Lesion
A Severe Calcified Lasting Artery Case: Percutaneous Coronary Intervention With Rotational Atherectomy
Trung Minh Tran1, Huynh Trung Cang1
Kien Giang General Hospital, Vietnam1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Medical history of the patient included coronary artery disease underwent percutaneous coronary intervention in left circumflex artery in 2017, chronic reduced enjection fraction heart failure in 2020, hypertension in 2016.Physical exam: patient had angina on exertion, dyspnea, 3/6 systolic murmur in apex and normal heart rate, low blood pressure, no rales in two lungs.
Relevant Test Results Prior to Catheterization
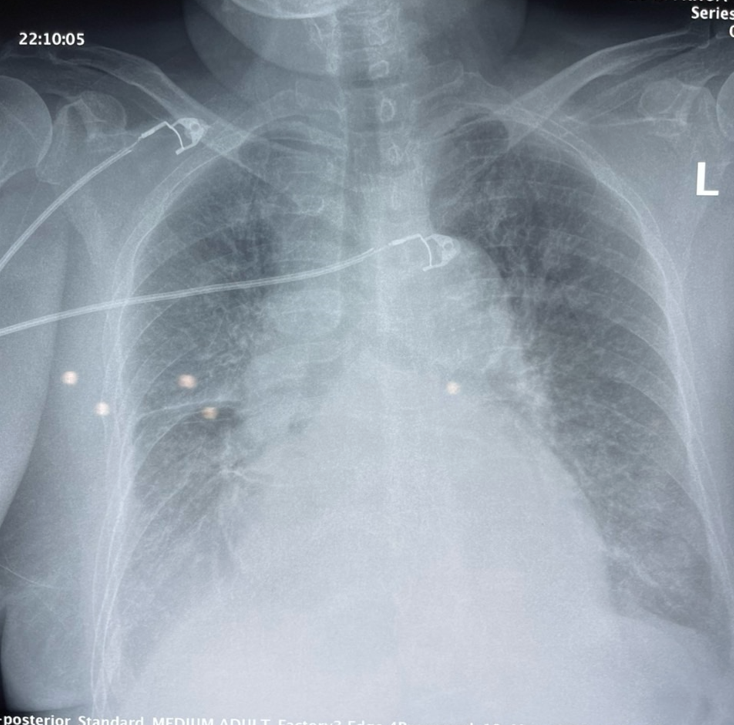
Electrocardiogram showed normal sinus rthythm with tachycardia, anterolateral ischemia.Echocardiogram showed dilated left ventricle of 69mm, reduced left ventricular ejection fraction of 15%, intermediate mitral regurgitation and intermediate to severe aortic regurgitation.Chest xray demonstrated mild lungs edema.Blood test showed elevated troponin I of 100 ng/mL and normal electrolyte tests.Abdominal echo showed old liver lesion.
Relevant Catheterization Findings
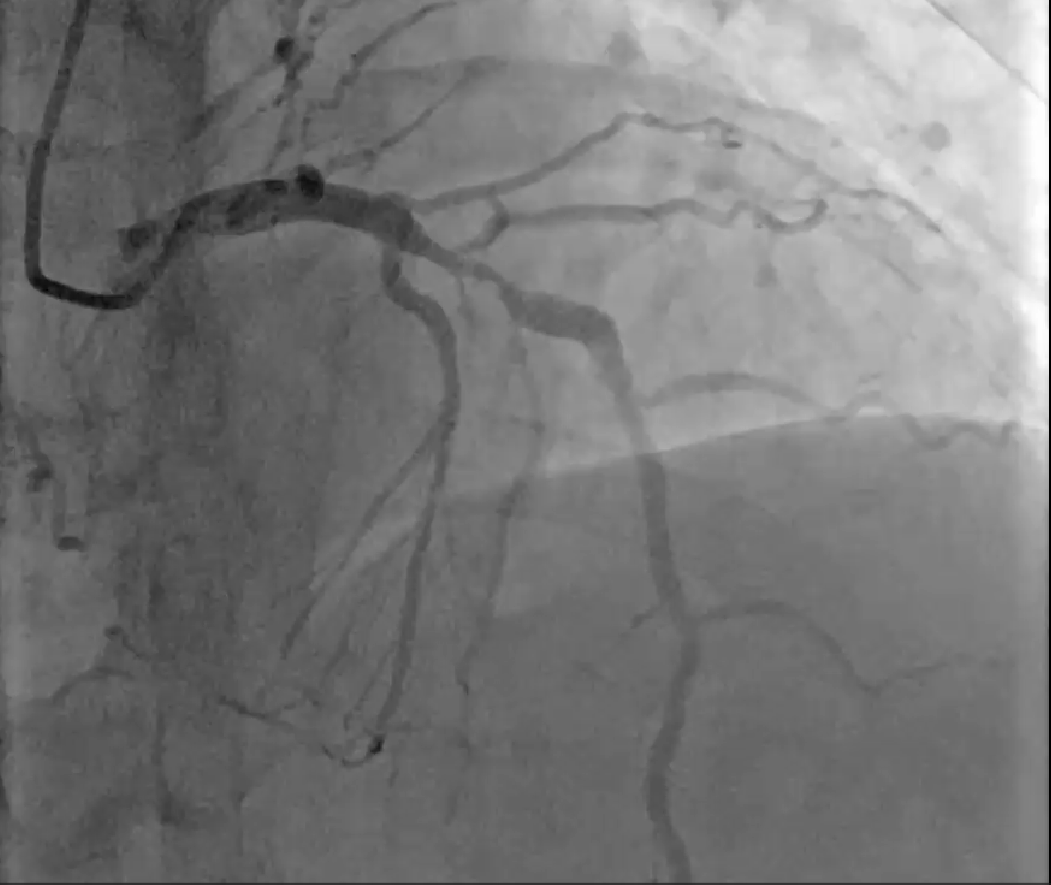
angiography showed 95% stenosis in mid left anterior descending with moderate to severe calcification, chronic total occlusion in left circumflex artery with microchanel collaterals and chronic total occlusion in-stent mid right coronary artery with left collaterals from first septal artery.


Interventional Management
Procedural Step
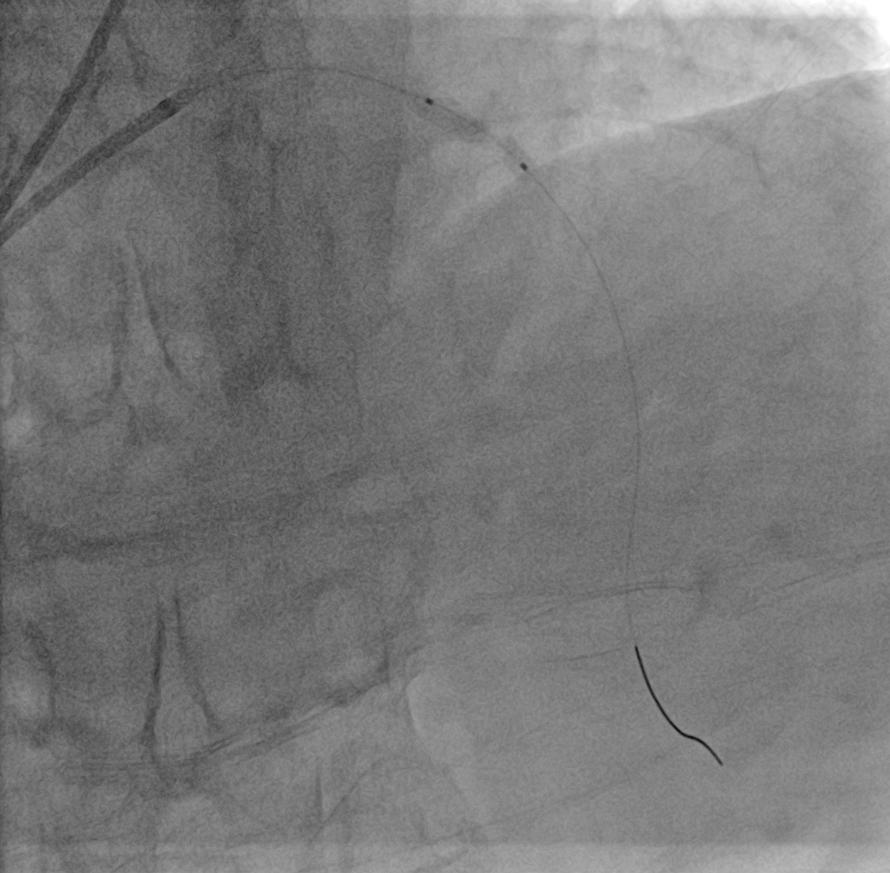
We had two stages in our case.First stageWe did radial artery access , EBU 3.5 6F guiding catheter, runthrough NS 0.014inch guidewire. After guidewire going through left anterior artery distally, we predilated 2.0*20 compliant balloon at 10atm, then 2.5*15 noncompliant balloon at 18atm but stent could not pass the lesion. So we decided to stop the procedure and did it again with rotational atherectomy.Second stageWe did femoral artery access, EBU 3.5 7F but two external iliac artery had significant stenosis. So we changed to radial artery access with EBU 3.5 6F. The first plan was to use 1.5mm burr, then changed to 1.25mm burr due to 6F guiding catheter. After rotawire going through mid left anterior descending artery, we advanced the rota burr with dynaglide mode and then did five times rotablator run, first run at 182000 r/min in 15 second, second run at 183000 r/min in 13 second, third run at 183000 r/min in 11 second , fourth run at 184000 r/min in 13 second and last run at 183000 r/min in 13 second. After that we predilated mid left anterior descending with 3.25*10mm noncompliant balloon at 10-12 atm. We deployed 4.0**23 DES stent in mid left anterior artery at 16atm (4.27mm). We did the final picture and had a good result.


Case Summary
we encountered a case having last remaining artery with significant calcified stenosis. We evaluated the situation with two aspect. Firstly, patient was stable and had supine position when we did percutaneous intervention. Secondly, although patient had two chronic total occlusion, but two collaterals from right coronary artery and left circumflex would not affected by left anterior descending intervention. We had a very good predilation at the first stage but the stent coud not pass the lesion. We thought that the severe calcified lesion and thanked to rotational atherectomy, we had good result after five rotablator runs and stenting.