
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-218
Valve-in-Ring Transcatheter Mitral Valve Replacement With LAMPOON Leaflet Modification Technique
By Ka-Chun Un, Eric Kwong Yue Chan, Tai-Leung Daniel Chan, Cheung Chi Simon Lam
Presenter
Ka-Chun Un
Authors
Ka-Chun Un1, Eric Kwong Yue Chan1, Tai-Leung Daniel Chan1, Cheung Chi Simon Lam1
Affiliation
Queen Mary Hospital, Hong Kong, China1,
View Study Report
TCTAP C-218
Structural - Mitral Valve Intervention - Transcatheter MV Replacement
Valve-in-Ring Transcatheter Mitral Valve Replacement With LAMPOON Leaflet Modification Technique
Ka-Chun Un1, Eric Kwong Yue Chan1, Tai-Leung Daniel Chan1, Cheung Chi Simon Lam1
Queen Mary Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
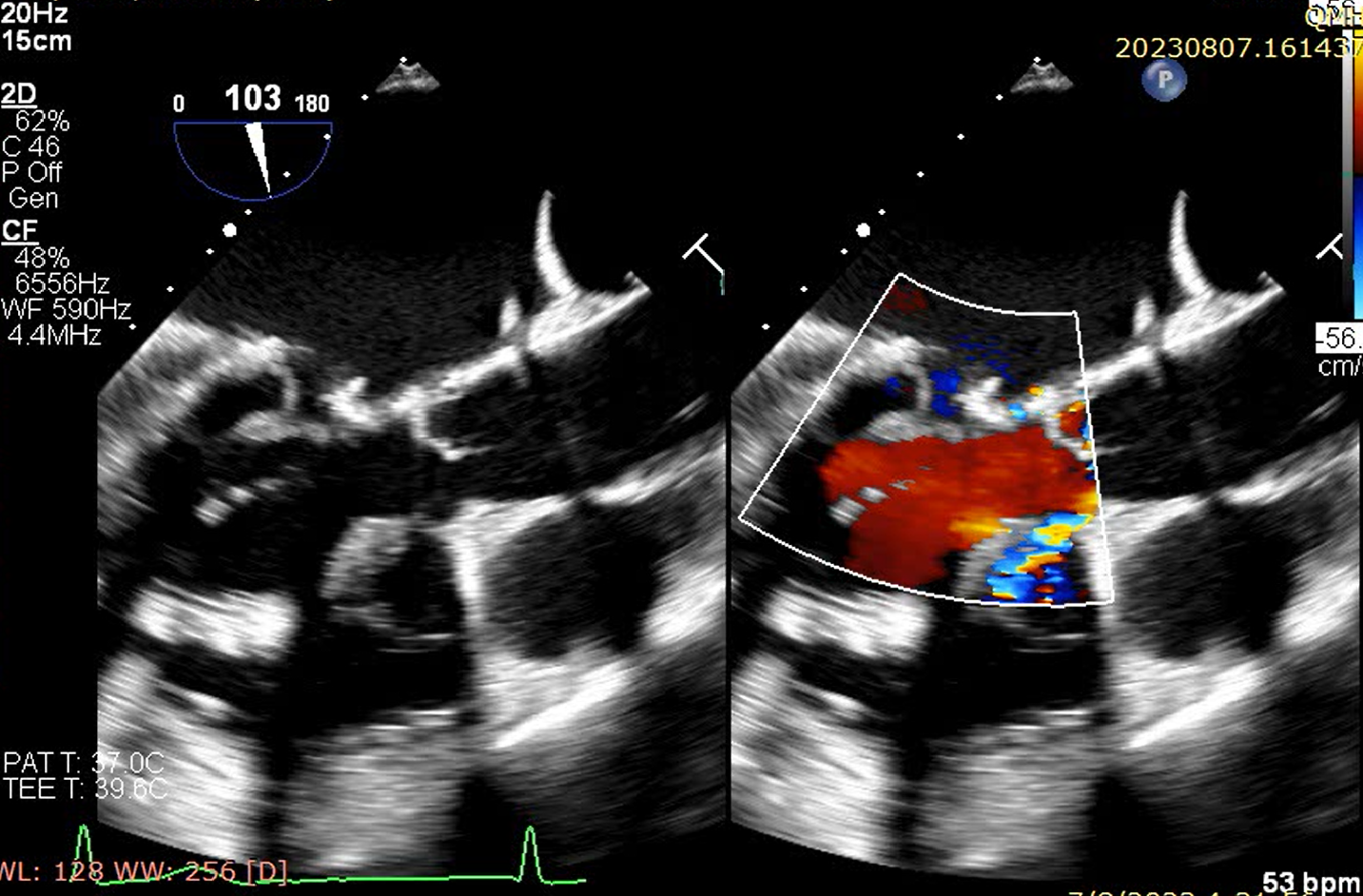
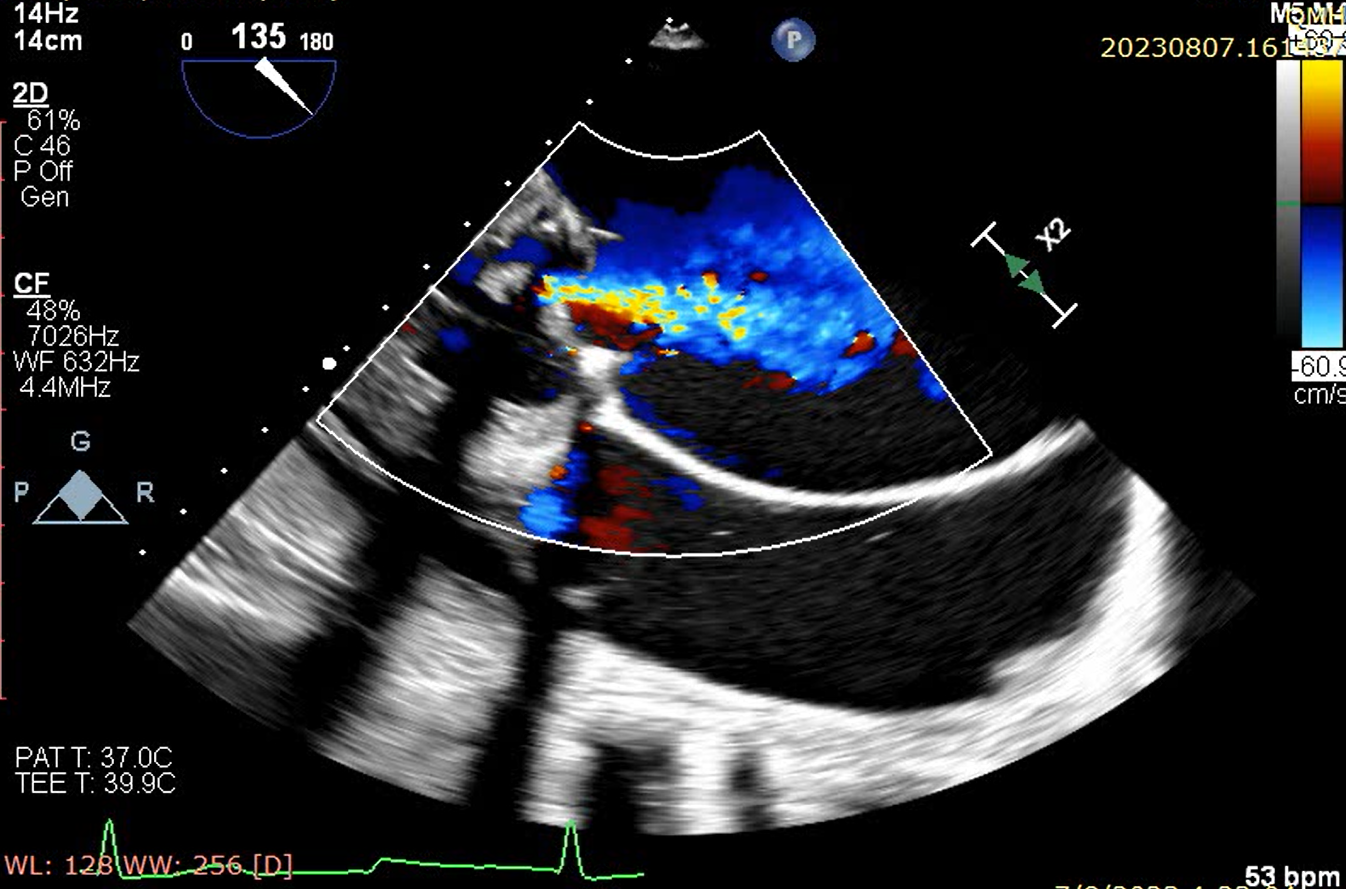
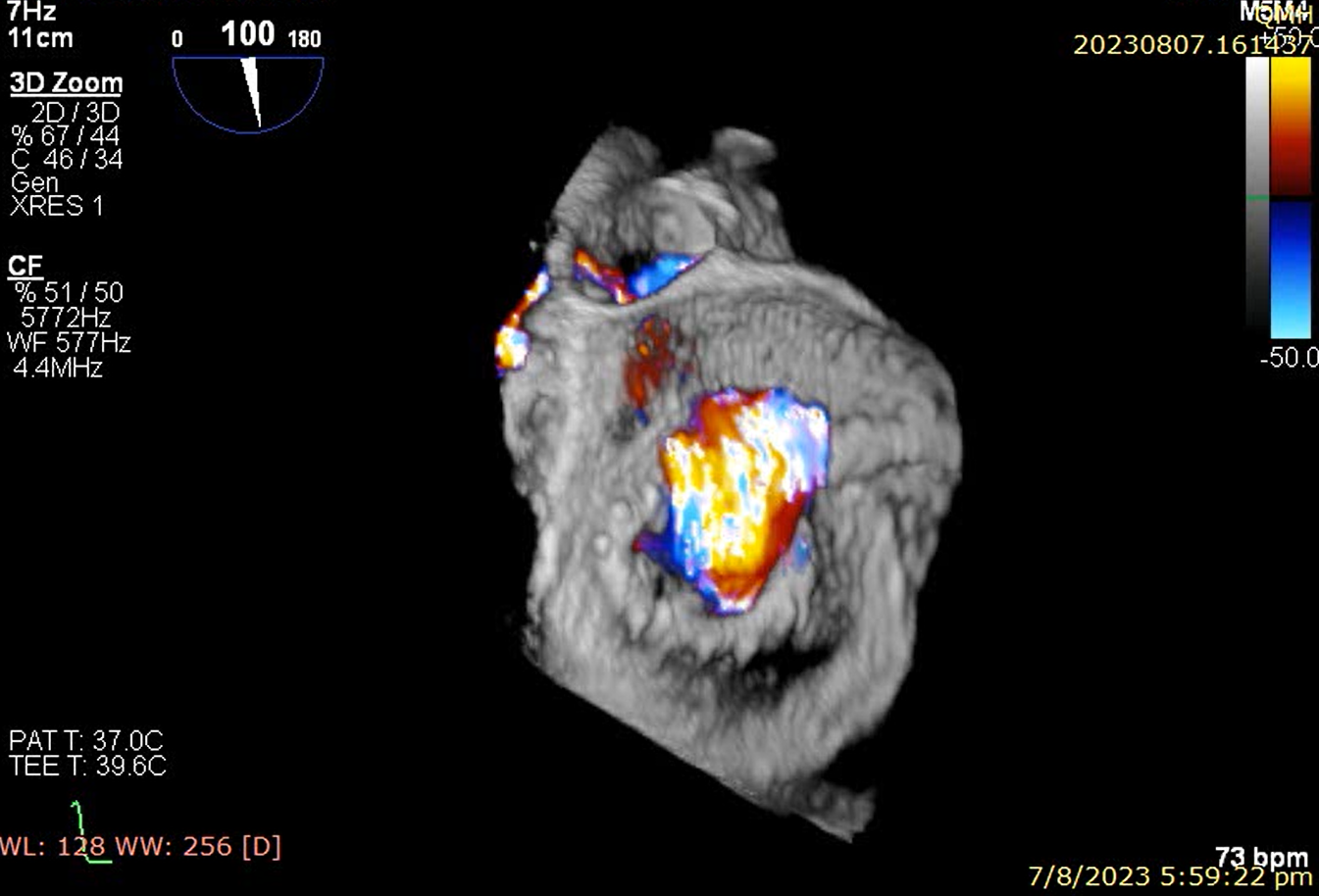
An 89-year-old lady with history of mitral valve repair has repeated admissions to the hospital for congestive heart failure. She has known chronic rheumatic heart disease requiring mitral valve repair with a Physio Ring 32 mm (Edwards Lifesciences, CA, USA) 13 years ago. Echocardiogram showed severe mitral regurgitation. The Heart Team has considered the patient to have prohibitive surgical risk and has recommended for a valve-in-ring transcatheter mitral valve replacement.

Relevant Test Results Prior to Catheterization
Blood test showed the creatinine level was 145 umol/L and the estimated glomerular filtration rate was 27 ml/min/1.73m2. The baseline N-terminal prohormone of brain natriuretic peptide was 1096 ng/L. Echocardiogram showed a dilated left ventricle with a preserved ejection fraction. The left atrium was severely dilated. There was severe transvalvular prosthetic mitral regurgitation with a raised mean gradient of 9 mmHg. Computerized tomography showed a borderline aortomitral angle.
Relevant Catheterization Findings
Interventional Management
Procedural Step
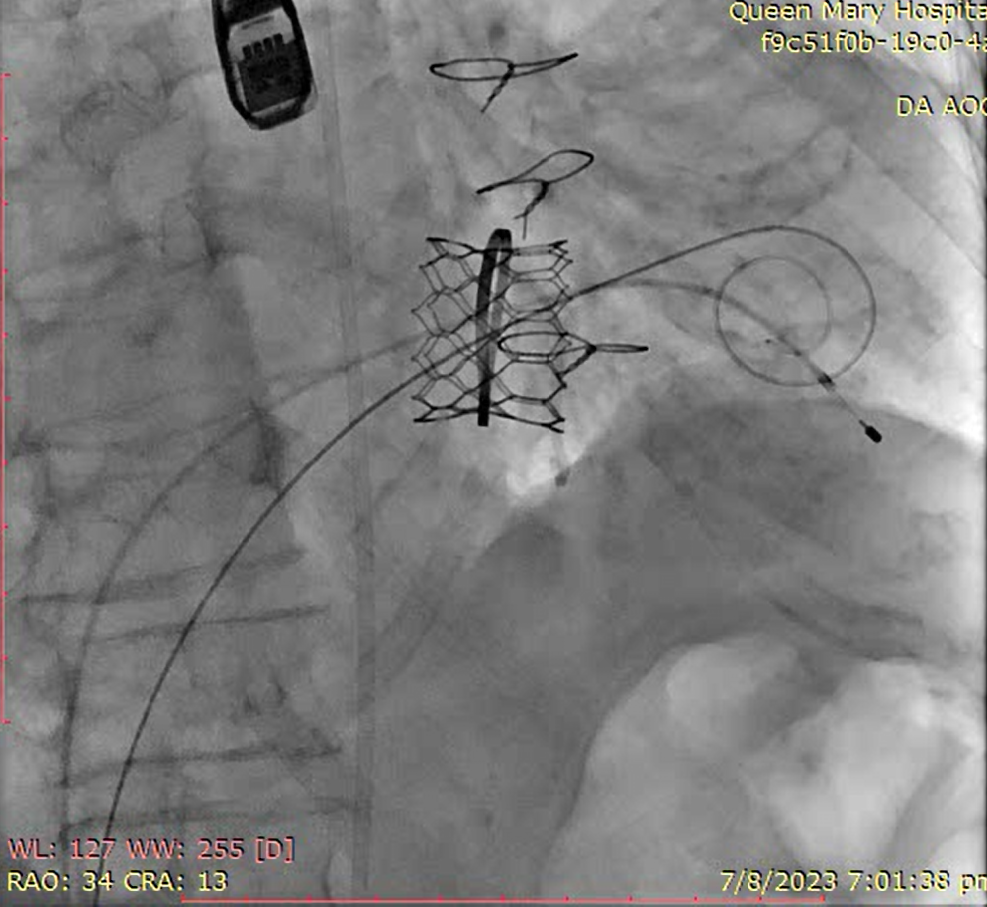
Transeptal puncture was performed and a steerable sheath was advanced into the left atrium. Tip-to-base intentional laceration of anterior mitral leaflet to prevent left ventricular outflow tract obstruction (LAMPOON) was planned. The mitral valve was crossed with a Swan-Ganz Catheter with an inflated balloon tip towards the left ventricular outflow tract (LVOT). An Astato HS 20 guidewire (Asahi Intecc, CA, USA) with a pre-formed flying V was delivered into the ascending aorta, followed by a Piggyback catheter with the tip just proximal to the Flying V. The distal end of the Astato wire was snared at the ascending aorta to form an arteriovenous (AV) loop and then externalized. Another Navicross catheter (Terumo, Japan) was introduced from the aortic end with a trapping balloon inside. With this set-up, the Astato wire was insulated by both the catheters at two ends with the middle flying V exposed. The flying V was moved to the mitral A2 position as seen on echocardiogram. Tip-to-base electrosurgical cutting with 70W for 2s was performed by gentle traction of the flying V. The anterior mitral valve leaflet was successfully split with worsening of regurgitation.

Case Summary
Left ventricular outflow tract obstruction secondary to displacement of the pre-existing anterior mitral valve leaflet has always been the Achilles heel of transcatheter mitral valve replacement. In selected patients with a prosthetic valve or ring, the tip-to-base LAMPOON leaflet modification technique could be effective in splitting the anterior mitral valve leaflet to mitigate this risk.