
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-184
A Challenging Case: Intravascular Ultrasound (IVUS) for Percutaneous Coronary Intervention (PCI) Guidance in Calcified, Tortuous and Giant Right Coronary Artery (RCA)
By Evi Supriadi Sukardi
Presenter
Evi Supriadi Sukardi
Authors
Evi Supriadi Sukardi1
Affiliation
Raden Matther General Hospital, Indonesia1,
View Study Report
TCTAP C-184
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
A Challenging Case: Intravascular Ultrasound (IVUS) for Percutaneous Coronary Intervention (PCI) Guidance in Calcified, Tortuous and Giant Right Coronary Artery (RCA)
Evi Supriadi Sukardi1
Raden Matther General Hospital, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 68-years-old, smoker male complained recurrent chest pain and shortness of breath mainly during activity for the past month, relieved by taking nitrates sublingually. History of treatment for coronary artery disease, hypertension, obesity, and dyslipidemia. He has been smoking for 40 years, one pack per day. Physical examination found compos mentis, BP of 156/100 mmHg, RR of 24 bpm, HR of 96 bpm, SpO2 94% with room air. Cardiopulmonary physical examination was normal.
Relevant Test Results Prior to Catheterization
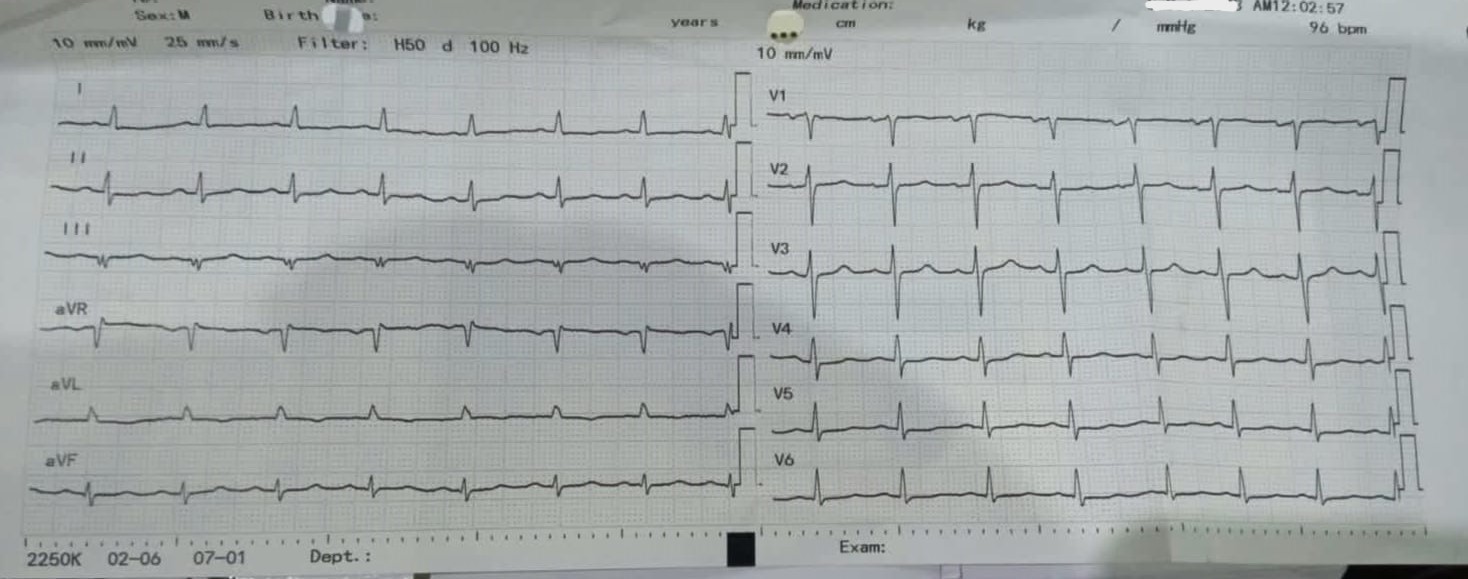
During the preparation for intravascular ultrasound (IVUS) - guided percutaneous coronary intervention (PCI) procedure, patient was reevaluated. There was no complaint of chest pain, physical examination showed BP 139/89 mmHg. ECG showed pathologic Q wave at leads III. Echocardiogram showed left ventricular (LV) systolic function was decreased (ejection fraction 36%), hypokinetic LV in infero-posterior, apical and lateral with mild regurgitation.
Relevant Catheterization Findings
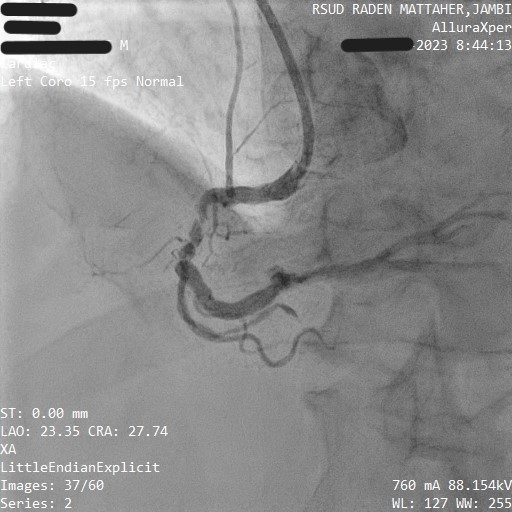
Coronary angiography was performed on October 20th, 2022, when patient suffered the first acute onset of cardiac ischemia, which showed giant right coronary artery (RCA) with 90% stenosis in proximal-mid RCA, and 85% stenosis in distal RCA, with calcification, and tortuous in the RCA. Based on these findings, it is preferred that the patient undergoes PCI with IVUS guidance, as IVUS can provide better visualization and aid in a better outcome.
Interventional Management
Procedural Step
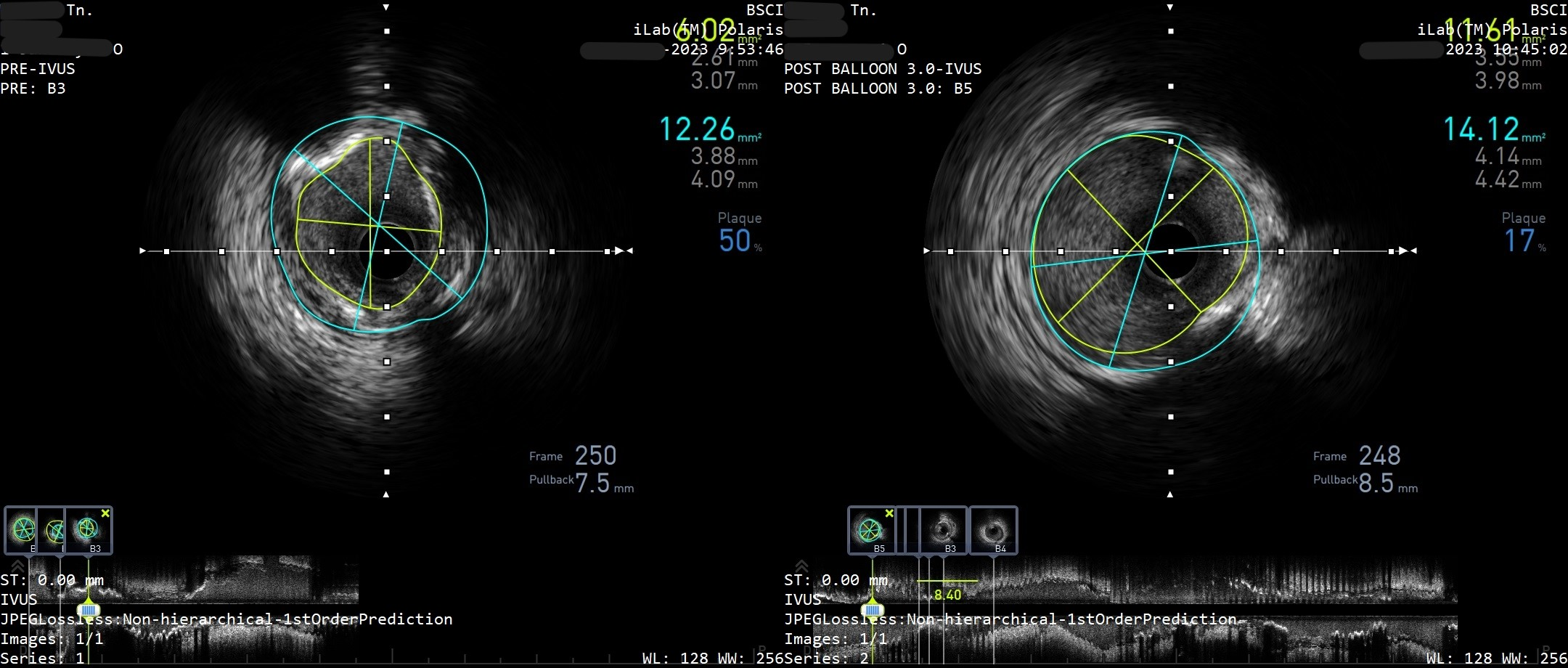
PCI was performed using sheath 6F and JR 3.5/6F catheter via trans-radial and showed giant and tortuous RCA with 90% stenosis in proximal-mid RCA and 85% stenosis in distal RCA. First IVUS showed severe calcification and fibrosis in distal RCA, but wire failed to penetrate the lesion. A second attempt of rewiring was successfully performed with RunthroughFloppy double wire, and the first stent (DES Biomatrix 3.5x14 mm) was inserted in distal RCA with pressure of dilatation approximately 12 atm. A second stent (Promus Premier 3.5x32 mm) was unable to pass the lesion in proximal-mid RCA. IVUS showed a similarly tortuous and diffuse calcification in proximal-mid RCA. GC Godzilla was used to successfully deliver the stent into place, dilated to 18 atm. The third and final stent (Promus Element 4.0x16 mm) was inserted in proximal RCA, overlapping with previous stent in proximal RCA. The third stent was placed to a good position and deployed with pressure of 14 atm. After this final stent was deployed, an evaluation of the stent installation was performed with angiography. Findings showed good outcome with TIMI flow III, and no dissection. Final IVUS demonstrated well-apposed stent in three locations of RCA: proximal, mid and distal. After the evaluation was completed, IVUS probe and all other tools were pulled out. The patient's hemodynamic was stable with BP 135/68 mmHg, HR 94 bpm, and complications such as dissection and perforation were not found during and after the procedures.

Case Summary
We have case about the challenging and successfully performed PCI procedure of three stents in RCA guided by IVUS in a 68-year-old male that was diagnosed coronary artery disease with stenosis and diffuse calcification in tortuous and giant RCA. IVUS was chosen and decided for guiding PCI procedure. Calcification and coronary tortuosity significantly increase the risk complication such as stent loss and artery dissection. IVUS play an important role to evaluate stent installation and to find out the complication after stenting, particularly in this challenging case.