
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-107
Entrapped in an Unexpected Site During Retrieval of Dislodged Coronary Stent
By Tsz Ho Chan, Wai Lun Mak, Chi Na Cheng, Yu Ho Chan, Shung Yee Wong, Chi Wing Wong
Presenter
Tsz Ho Chan
Authors
Tsz Ho Chan1, Wai Lun Mak1, Chi Na Cheng1, Yu Ho Chan2, Shung Yee Wong1, Chi Wing Wong1
Affiliation
Pok Oi Hospital, Hong Kong, China1, The CUHK Medical Centre, Hong Kong, China2,
View Study Report
TCTAP C-107
Coronary - Complication Management
Entrapped in an Unexpected Site During Retrieval of Dislodged Coronary Stent
Tsz Ho Chan1, Wai Lun Mak1, Chi Na Cheng1, Yu Ho Chan2, Shung Yee Wong1, Chi Wing Wong1
Pok Oi Hospital, Hong Kong, China1, The CUHK Medical Centre, Hong Kong, China2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
The patient was presented to us with CCS Class 3 stable effort angina. She suffered from hypertension, diabetes mellitus, hyperlipidemia, and a history of thyroidectomy for goiter. She underwent CTCA and showed positive results. Despite of trial of anti-anginal medications, she was still symptomatic. Therefore she was offered to have elective coronary angiogram +/- percutaneous coronary intervention. Her physical examination was unremarkable. ECG showed poor R-wave progression

Relevant Test Results Prior to Catheterization
CTCA showed
calcium score of 475. RCA Dominant.
LM: mild disease
LAD: pLAD 50%, diffuse 0-25% disease
LCX: pLCX 0-25%, dLCx 0-25% disease
RCA: pRCA 0-25%
Echo showed normal chamber size with satisfactory bi-ventricular systolic function
LVEF 60% without regional wall motion abnormalities
trileaflet aortic valve without significant valvular pathology
No pericardial effusion
Relevant Catheterization Findings
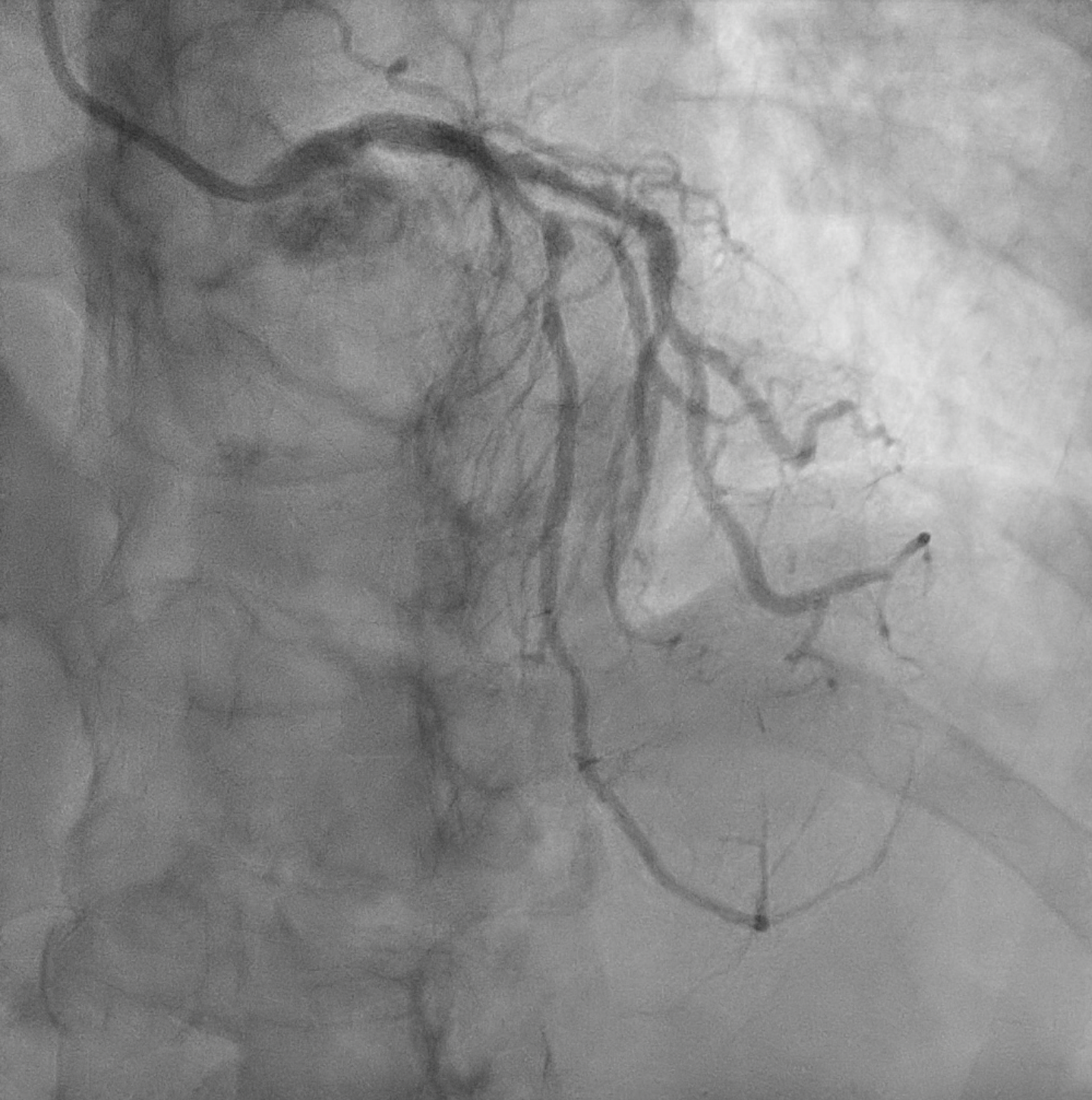
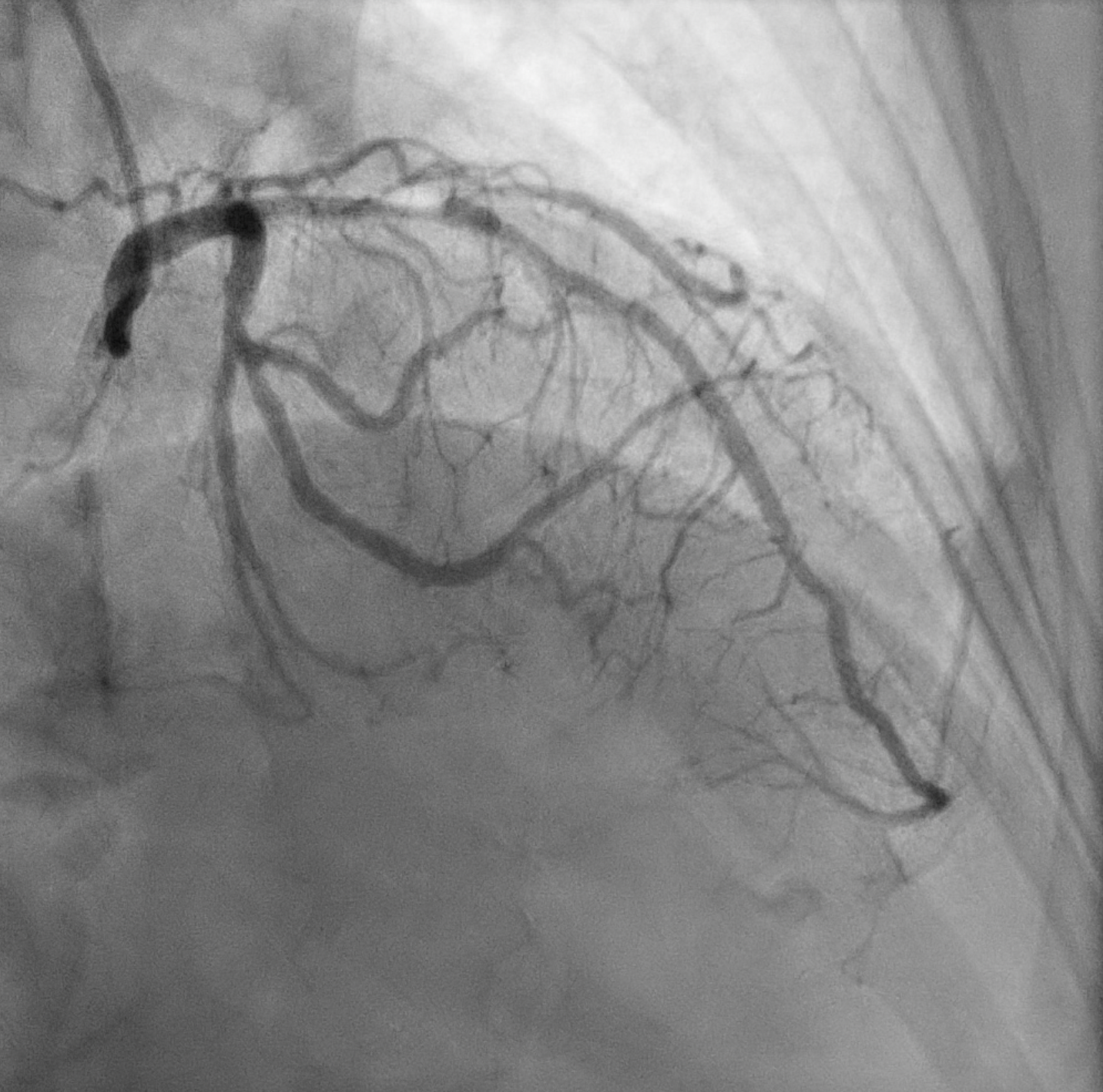
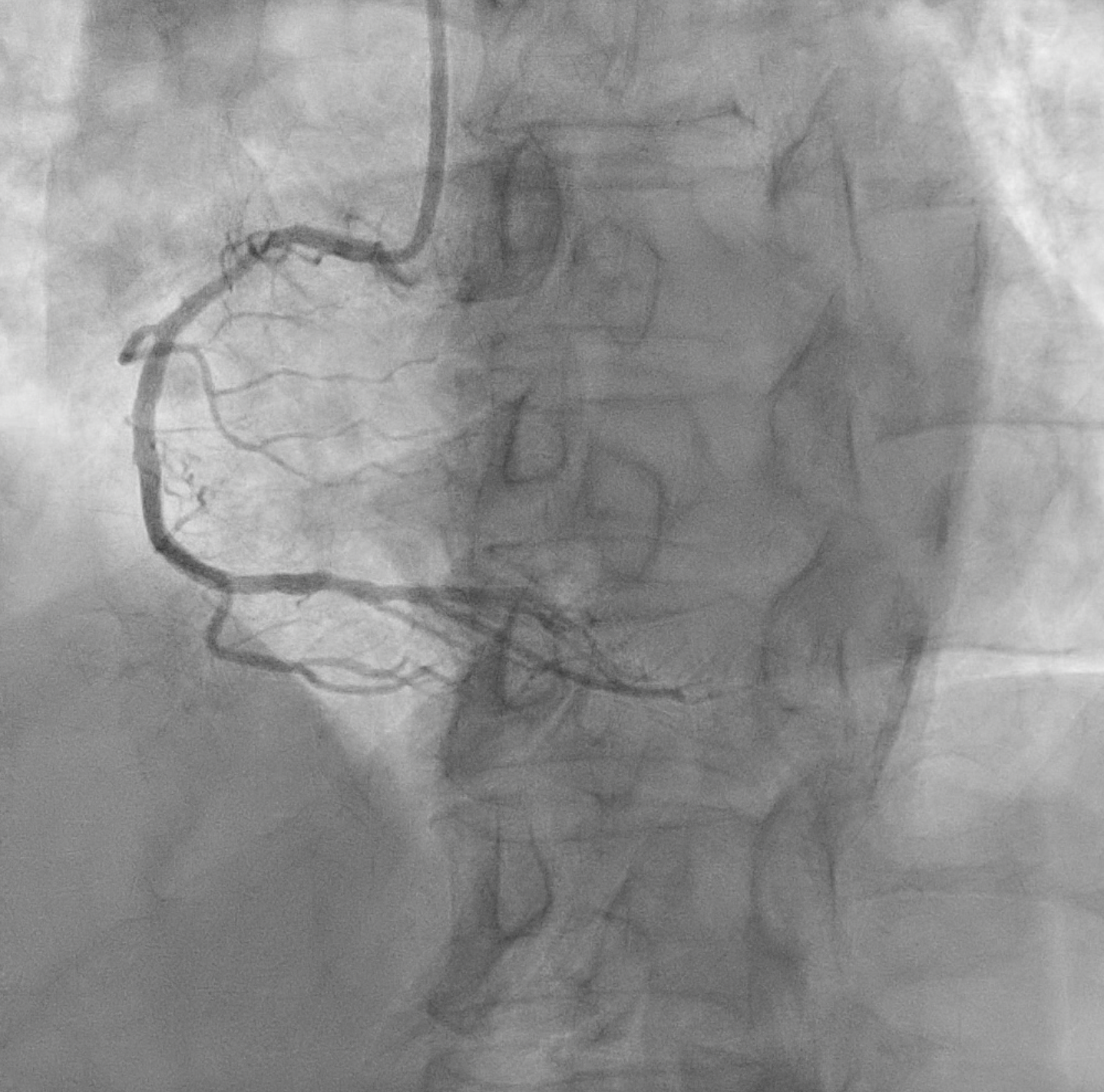
Left main : Normal LAD: severe proximal-mid LAD with D1 bifurcation lesion ( Medina 1,1,1 ) and diffuse mild diseaseLCX: mild to moderate 40% at mid LCX RCA: Dominant, severe 70% proximal RCA disease
Interventional Management
Procedural Step
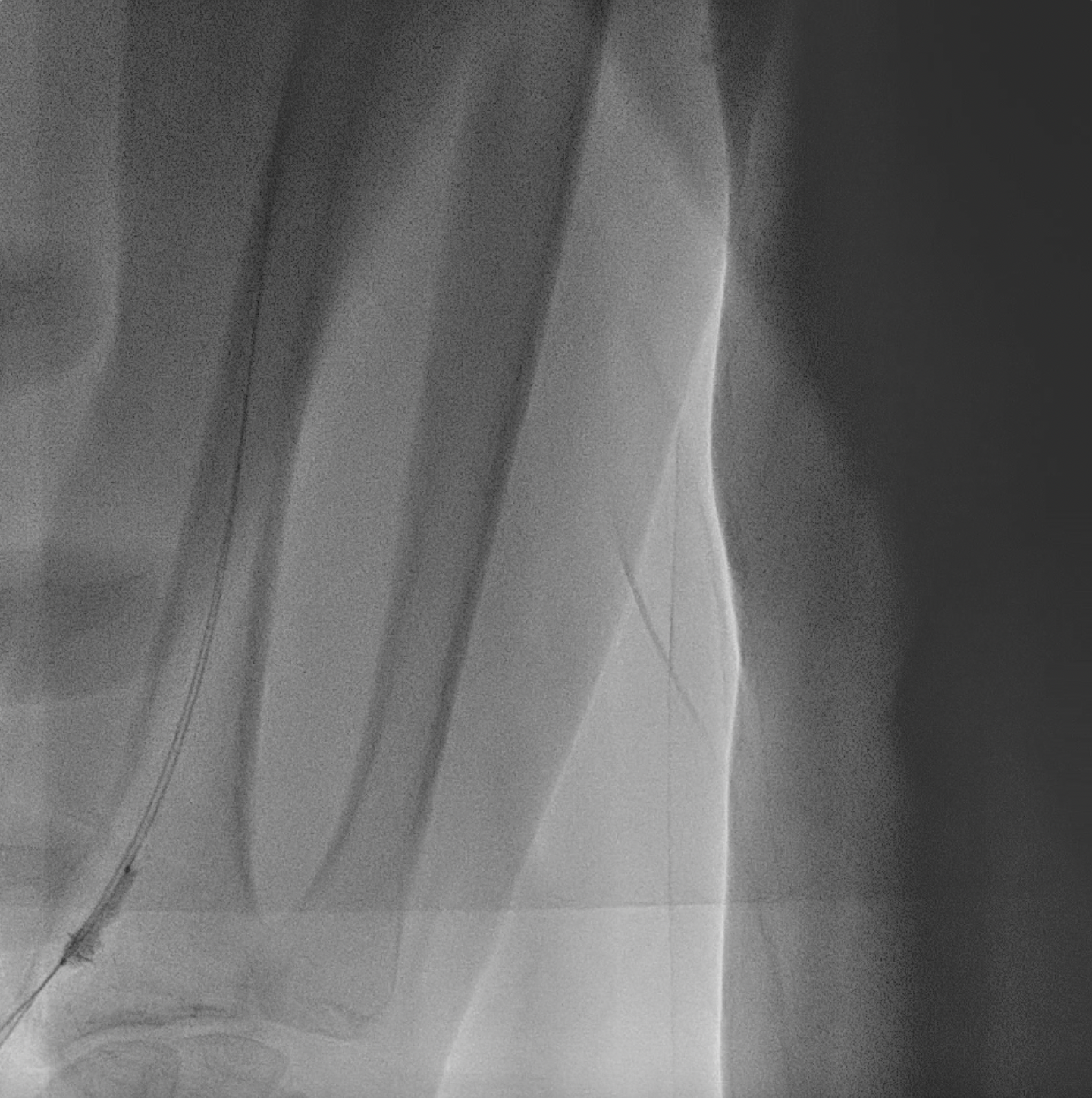
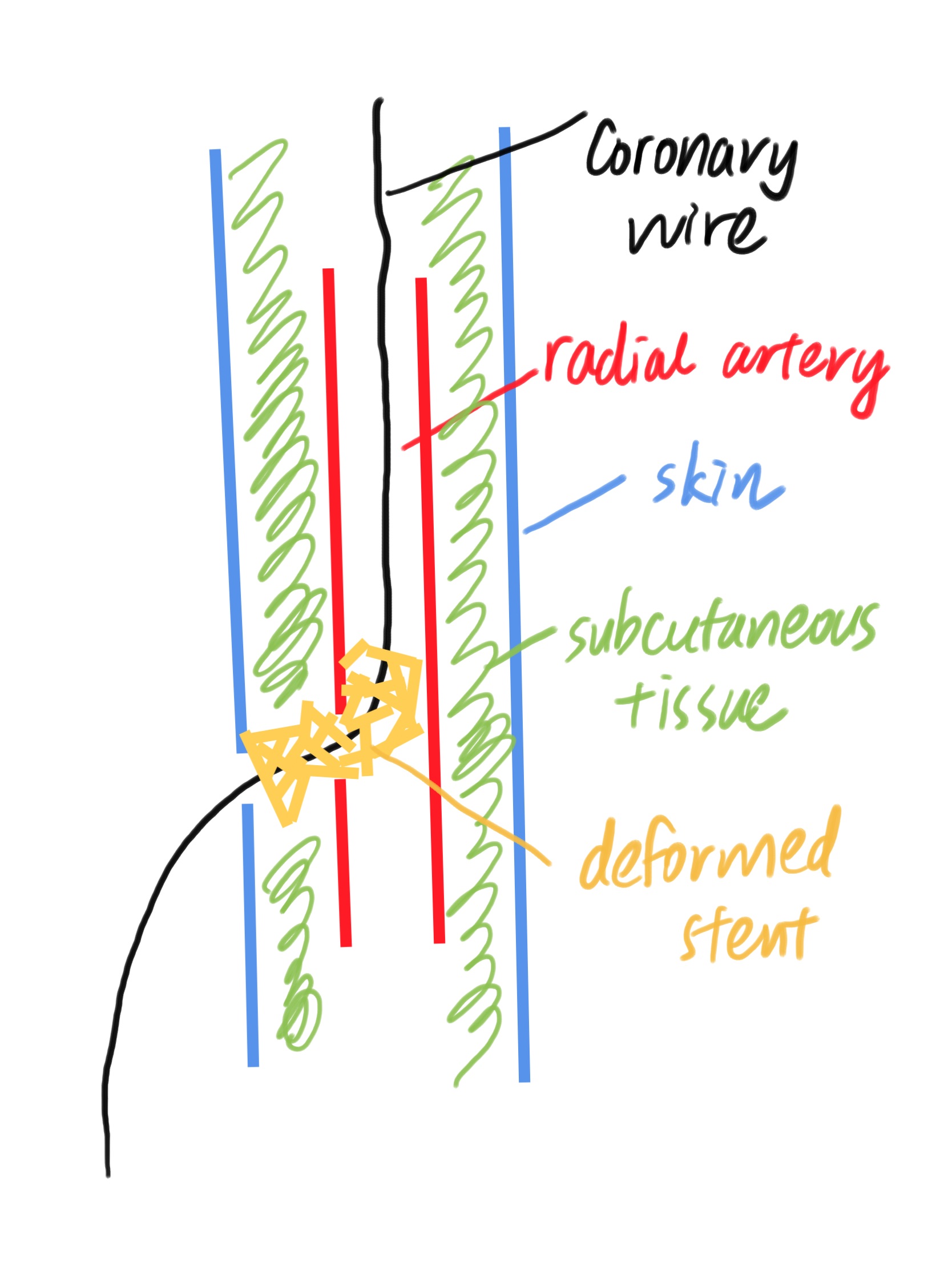
The case underwent PCI with Fr 6 EBU 3.5 with the right radial approach. Wiring to LAD and D1 was done and OCT was used for lesion analysis. Lesions were pre-dilated with semi-compliant and cutting ballon. During the advancement of a stent to D1 stent dislodgement. Small-sized balloon was advanced past the dislodged stent and attempted to pull back the stent. The stent was not able to retrieve the guiding catheter completely. IVUS showed the stent partially inside the guiding catheter. We decided to remove the stent and guide it as a whole with a balloon inflated distal to the stent. At first, the stent was trapped in the proximal part of the radial artery. After vasodilators and analgesics, the stent was brought to the distal radial artery. However, the stent was trapped inside the radial artery despite attempts to pull the stent inside the sheath with balloon inflated distally. We locate the stent by fluoroscopy by a radio-opaque balloon outside the body, showing close to the puncture site. We inflated the pressured cuff at the upper arm and the stent was removed under direct vision with a slight exploration
We continued the procedure with the same radial artery access after checking circulation. The LAD/D1 lesion was managed with DK Crush technique with stenting done across LM-LAD-LCX. Because of the prolonged procedure, we decided to offer staged PCI to RCA
In staged PCI left system showed no significant ISR. The patient was symptom-free and palpable radial artery in FU.

We continued the procedure with the same radial artery access after checking circulation. The LAD/D1 lesion was managed with DK Crush technique with stenting done across LM-LAD-LCX. Because of the prolonged procedure, we decided to offer staged PCI to RCA
In staged PCI left system showed no significant ISR. The patient was symptom-free and palpable radial artery in FU.
Case Summary
The case demonstrated the need for lesion preparation and avoidance of forceful pushing of the stent if resistance is felt. If the stent is not able to be retrieved back to the guiding catheter by pulling back the inflated distal balloon, think of other possible strategies before removing the whole catheter system. If needed, consider the use of vasodilators while pulling back the stent to the distal radial artery. Stent may be trapped inside the artery or subcutaneous tissue especially if it is deformed. A radio-opaque tool can be used to locate the trapped stent which in this case minimal puncture wound exploration is able to retrieve the stent without the need for operation.