
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-146
Drug Coated Balloon in de Novo Lesion of Large Coronary Vessel Lesion, Ostial Left Anterior Descending Artery (LAD): Should We Use It More?
By Jin Kiang Cheng, Wee Pang Ng, Mahadevan Gurudevan, Azrina Abdul Kadir, Jian Hao Sim, Richard Chay Shien Long
Presenter
Jin Kiang Cheng
Authors
Jin Kiang Cheng1, Wee Pang Ng2, Mahadevan Gurudevan3, Azrina Abdul Kadir2, Jian Hao Sim2, Richard Chay Shien Long4
Affiliation
Hospital Sultanah Aminah, Malaysia1, Sultanah Aminah Hospital, Malaysia2, Sultanah Amina Hospital, Malaysia3, Sultanah Aminah Hospital,, Malaysia4,
View Study Report
TCTAP C-146
Coronary - DES/BRS/DCB
Drug Coated Balloon in de Novo Lesion of Large Coronary Vessel Lesion, Ostial Left Anterior Descending Artery (LAD): Should We Use It More?
Jin Kiang Cheng1, Wee Pang Ng2, Mahadevan Gurudevan3, Azrina Abdul Kadir2, Jian Hao Sim2, Richard Chay Shien Long4
Hospital Sultanah Aminah, Malaysia1, Sultanah Aminah Hospital, Malaysia2, Sultanah Amina Hospital, Malaysia3, Sultanah Aminah Hospital,, Malaysia4,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
49 years old gentleman, ex-smoker, had history of acute anteroseptal myocardial infarction (November 2022), Killip 1, TIMI score 1, successfully thrombolysis with IV infusion streptokinase. During follow up, he is Canadian Cardiovascular Society (CCS) Angina Grade 1 with complained of mild symptoms angina with strenuous and prolonged exertion. He is hemodynamically stable with blood pressure 120/78 mmHg, manual pulse showed regular rhythm with 88 bpm. Physical examination showed unremarkable.
Relevant Test Results Prior to Catheterization
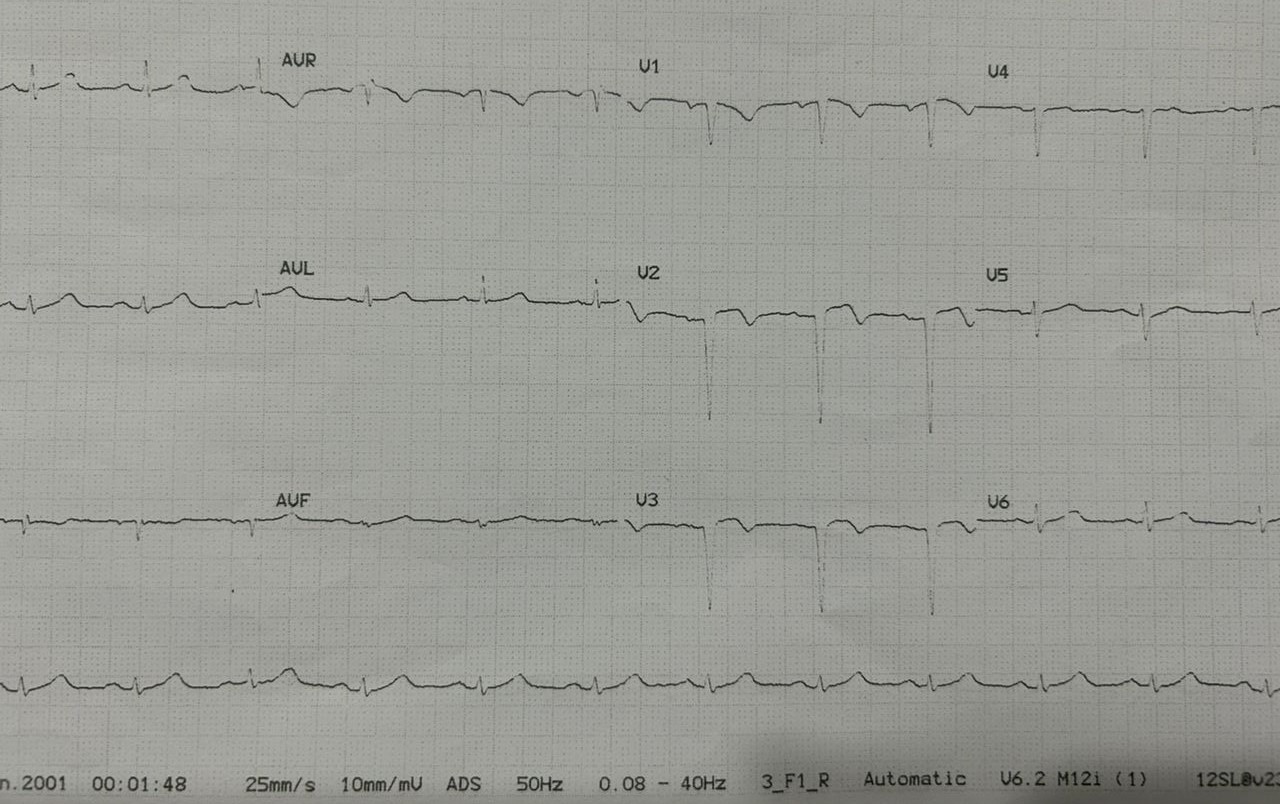
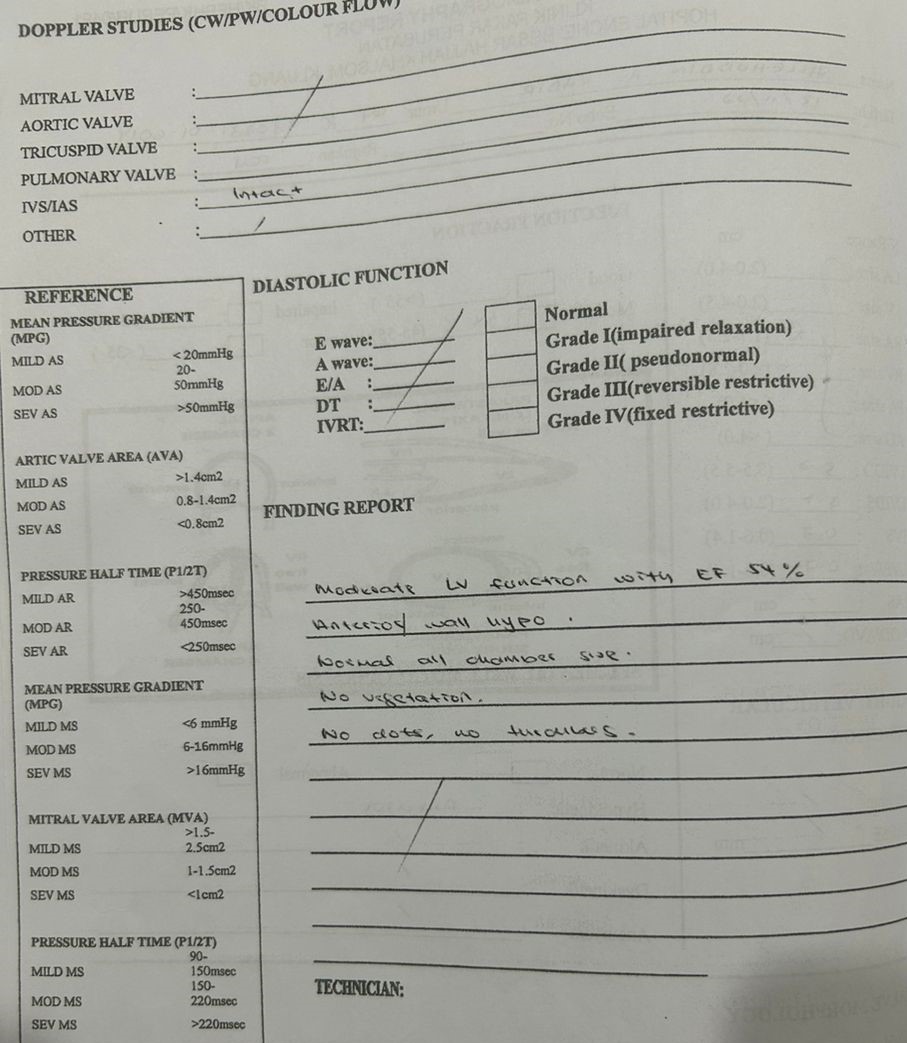
ECG showed sinus rhythm with Q wave anteroseptal region, T inversion V1 to V3. Echocardiogram showed normal LV function with EF 54%, anterior wall hypokinesia, normal chamber, all cardiac valve thin well coaptation, no regurgitation and stenosis, no clot or thrombus, no pericardial effusion.

Relevant Catheterization Findings
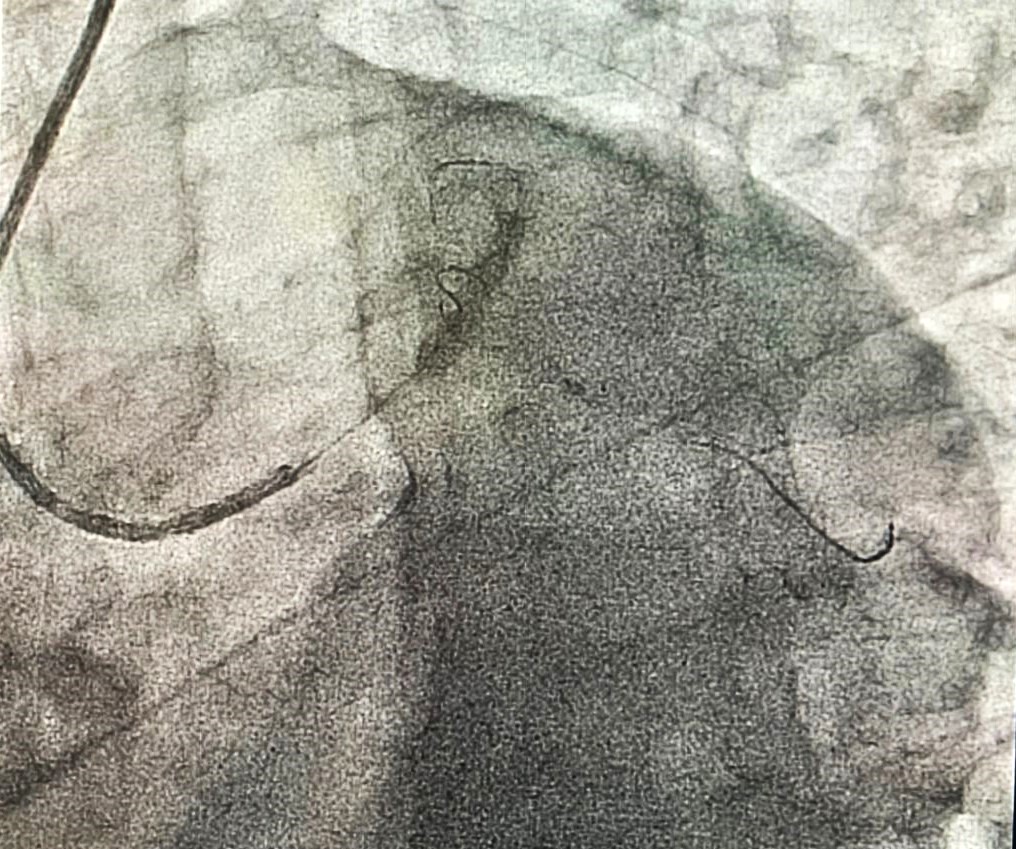
He had diagnostic coronary angiography on 21/5/2023, which showed a single vessel disease (SVD) with ostial left anterior descending artery (LAD) 95 % stenosis, with post stenosis aneurysmal and mild disease in distal LAD (20%). Mid left circumflex artery showed mild coronary artery disease with 20 % stenosis which is also aneurysmal. He has a high branch of first obtuse marginal artery(OM1) where proximal of OM1 showed 30% stenosis. He had a normal Right coronary artery vessel.



Interventional Management
Procedural Step
Percutaneous Coronary intervention was done via 6 Fr right radial approach. Total of IA 8000 units heparin and 300 mg oral clopidogrel given. Left coronary system was engaged with 6 Fr EBU 3.0 mm, successfully wired down to distal LAD with balance middleweight guide wire (BMWII J Tip). We tried to Pre-dilate ostial LAD with non-compliant (NC) balloon3.5 mm x 15 mm but unfortunately was unable to pass through tight lesion in ostial left anterior descending artery (LAD). So, we used a smaller size semi-compliant (SC) balloon 2.5 mm x 15 mm. We then predilate further with NC balloon 3.5 mm x 15 mm. It was able to cross the tight lesion of ostial left anterior descending artery (LAD), with slow and prolonged inflation and up to24 ATM, equivalent to 3.65 mm size. Lesion was well predilated to 1:1 ratio with no flow-limiting dissection, we proceeded to deploy Paclitaxel Drug coated balloon, PREVAIL 4.0 mm x 20 mm, up to 8 ATM, for 1 minute. Final result showed acceptable result with residual stenosis 30% and was end with total contrast used 100 cc, screening time 25 mins. He was discharged well next day with dual antiplatelet for 3 months. He remained asymptomatic and re-look coronary angiography after 3 months (August 2023), showed positive remodeling of ostial left anterior descending coronary artery (LAD) with no new lesion in other coronaries vessel. Patient remained completely asymptomatic.


Case Summary
Reason for choosing a Drug Coated Balloon is due to a size discrepancy in post stenotic aneurysm which poses risk of inadequate stent opposition and expansion if we were to implant a stent and higher risk of in-stent restenosis. Besides, we do not have self- expandable stent to allow optimal adaptation of the stent struts to the vessel wall in order to reduce the occurrence of stent malposition. Although evidence of DCB in de novo large and ostial lesion is limited but examples of studies shown promising and good results as compare to DES. We had demonstrated good clinical and angiographic outcome in de novo ostial post-stenotic aneurysmal LAD stenosis.