
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-125
Stuck HD-IVUS Catheter During Coronary Angioplasty - How to Bailout
By Yue Hin Tang, Ho Fai Daniel Fong
Presenter
Yue Hin Tang
Authors
Yue Hin Tang1, Ho Fai Daniel Fong1
Affiliation
Princess Margaret Hospital, Hong Kong, China1,
View Study Report
TCTAP C-125
Coronary - Complication Management
Stuck HD-IVUS Catheter During Coronary Angioplasty - How to Bailout
Yue Hin Tang1, Ho Fai Daniel Fong1
Princess Margaret Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Our patient is a 63 years old gentleman with known past history of hypertension, T2DM, hypercholesterolemia. He is a non-smoker.
He was admitted to our hospital for unstable angina, suffering from chest pain for 1 month prior to hospitalization with increasing frequency. He had a private CT coronary angiogram done showing triple vessel disease with high calcium score (significant stenosis in proximal and mid LAD, proximal LCx, proximal and mid RCA).
Physical examination was unremarkable
He was admitted to our hospital for unstable angina, suffering from chest pain for 1 month prior to hospitalization with increasing frequency. He had a private CT coronary angiogram done showing triple vessel disease with high calcium score (significant stenosis in proximal and mid LAD, proximal LCx, proximal and mid RCA).
Physical examination was unremarkable
Relevant Test Results Prior to Catheterization
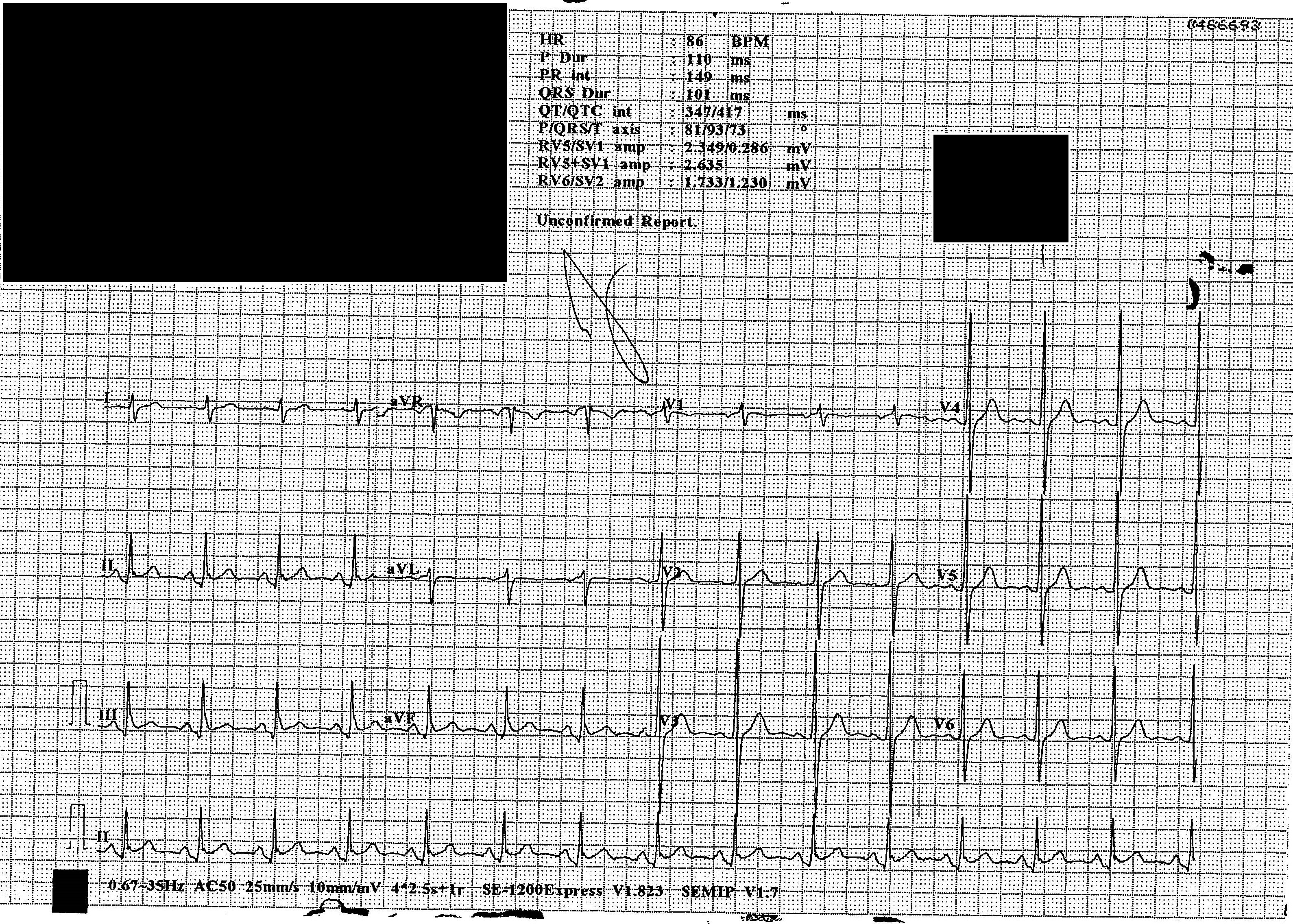
ECG showed sinus rhythm with no acute ischemic changesRepeated blood tests for elevated cardiac troponin came back negative.Transthoracic echocardiogram showed normal left ventricular systolic function without regional wall motion abnormality.
Relevant Catheterization Findings
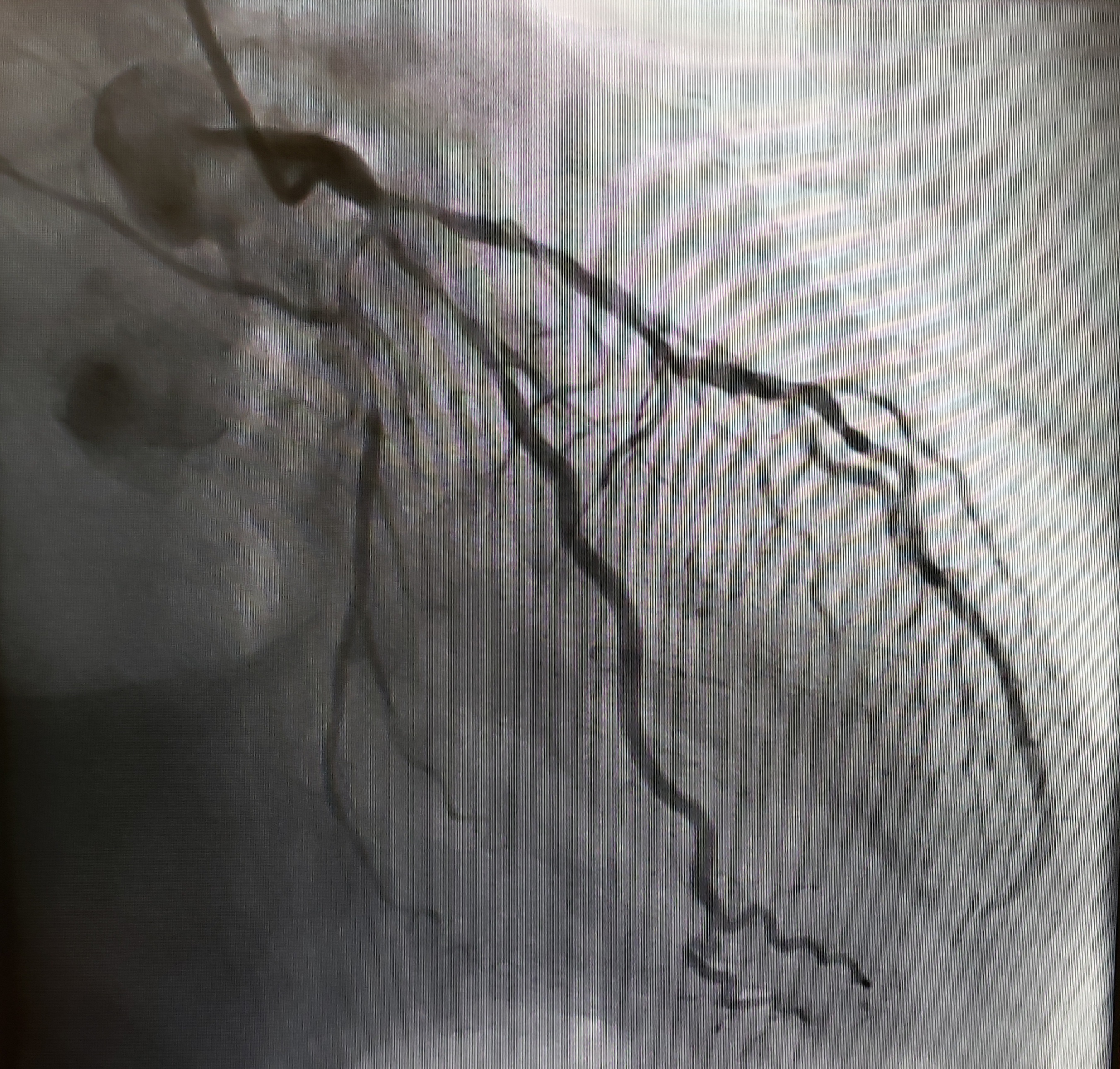
Diagnostic coronary angiogram showed a right dominant system, with involvement of left main and triple vessel disease.
Breakdown as followdistal LM 70%LAD diffuse calcified vessel with proximal LAD 80% stenosisproximal Ramus 90% stenosisproximal LCx 90% stenosis but small vesselproximal RCA 50%
Breakdown as followdistal LM 70%LAD diffuse calcified vessel with proximal LAD 80% stenosisproximal Ramus 90% stenosisproximal LCx 90% stenosis but small vesselproximal RCA 50%
Interventional Management
Procedural Step
Left coronary system was engaged with 7Fr EBU 3.5 guiding catheter.
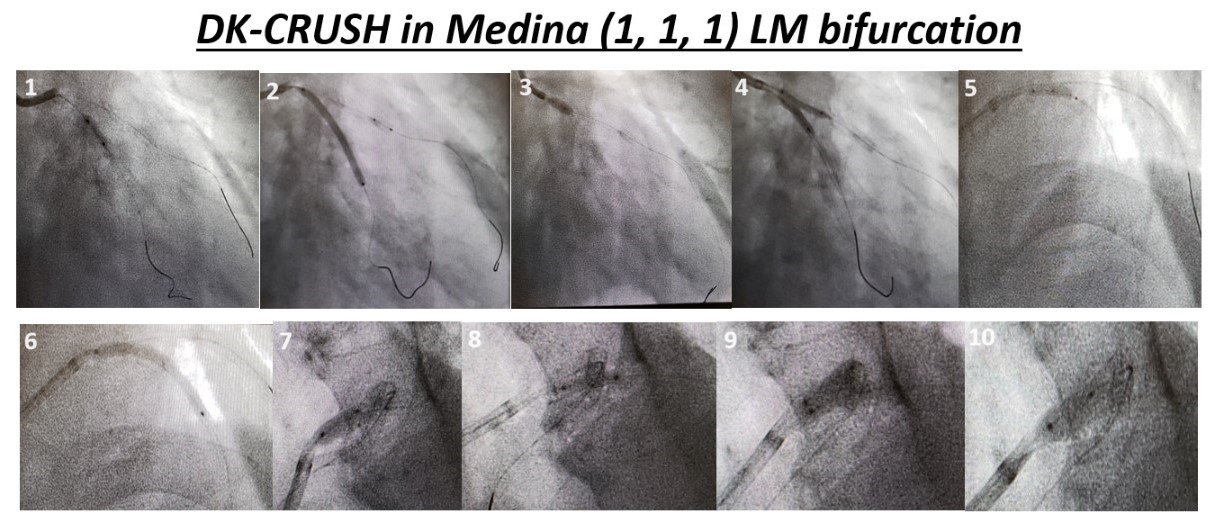
Our initial strategy was upfront LM/LAD/LCx bifurcation stenting by DK-CRUSH plus drug-eluting balloon to Ramus.
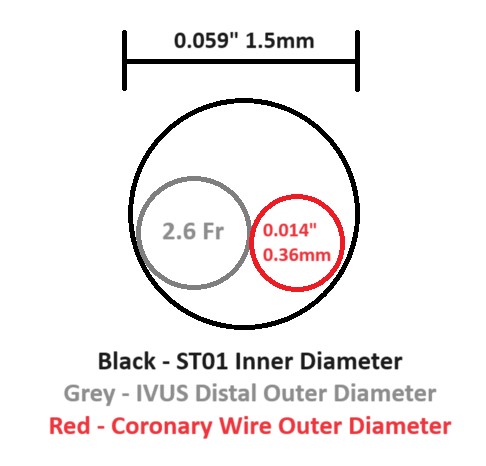
We proceeded according to the standardized steps for performing DK-CRUSH. The whole process was under intravascular ultrasound (HD-IVUS) guidance and it went smoothly.We then performed post-stenting IVUS study. Unfortunately, the IVUS got stuck after studying Ramus and was unable to be retrieved. We immediately stopped pulling. Then we tried different maneuvers for rescuing stuck IVUS.
We then completed the remaining part of the procedure uneventfully.

Our initial strategy was upfront LM/LAD/LCx bifurcation stenting by DK-CRUSH plus drug-eluting balloon to Ramus.
We proceeded according to the standardized steps for performing DK-CRUSH. The whole process was under intravascular ultrasound (HD-IVUS) guidance and it went smoothly.We then performed post-stenting IVUS study. Unfortunately, the IVUS got stuck after studying Ramus and was unable to be retrieved. We immediately stopped pulling. Then we tried different maneuvers for rescuing stuck IVUS.
We then completed the remaining part of the procedure uneventfully.
Case Summary
According to Murphy's Law, anything that can go wrong will go wrong.It is inevitable that interventional cardiologists come across complications during procedures as long as they perform interventions on patients. Of course being able to avoid complications from happeneing will be ideal, but sometimes it is not the case. Therefore it is of paramount importance to be well-preparaed for every possible outcome and to embrace the knowledge and techniques to get yourself out of the difficult situation should it really occur.Our case illustrated different methods used to retrieve stuck HD-IVUS catheter and we hope to share our experience and knowledge in this topic with colleagues worldwide.