
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-050
It’s a Bird! It’s a Plane! It’s Supercross!
By Aaron Hean Jin Ong, Muhamad Ali SK Abdul Kader, Imran Zainal Abidin
Presenter
Aaron Hean Jin Ong
Authors
Aaron Hean Jin Ong1, Muhamad Ali SK Abdul Kader2, Imran Zainal Abidin3
Affiliation
Hospital Sultan Idris Shah, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2, University Malaya Medical Centre, Malaysia3,
View Study Report
TCTAP C-050
Coronary - Complex PCI - CTO
It’s a Bird! It’s a Plane! It’s Supercross!
Aaron Hean Jin Ong1, Muhamad Ali SK Abdul Kader2, Imran Zainal Abidin3
Hospital Sultan Idris Shah, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2, University Malaya Medical Centre, Malaysia3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 39-year-old gentleman with hypertension, dyslipidaemia and aspirin allergy was staged for percutaneous coronary intervention (PCI) to left circumflex artery (LCx) chronic total occlusion (CTO) following a failed attempt 3 months ago. He has exertional angina with Canadian Cardiovascular Society (CCS) angina class II. He had no heart failure symptoms and was hemodynamically stable. Physical examination was unremarkable.

Relevant Test Results Prior to Catheterization
Haemoglobin level 13.6 g/dl
Relevant Catheterization Findings
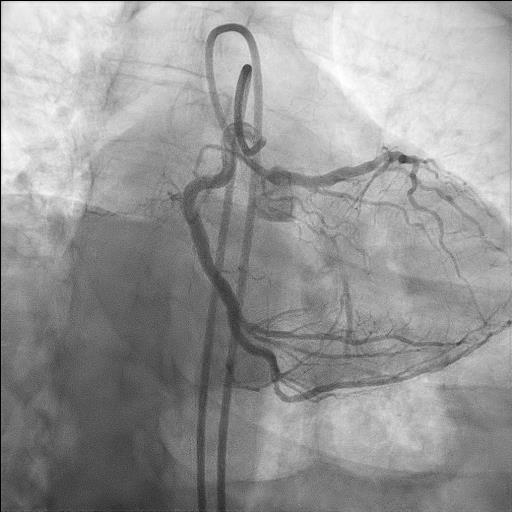
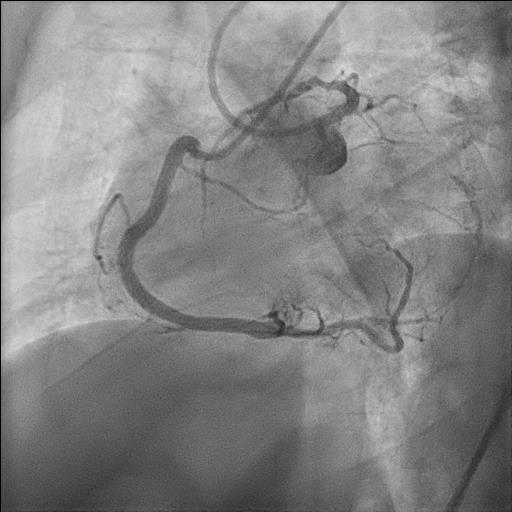
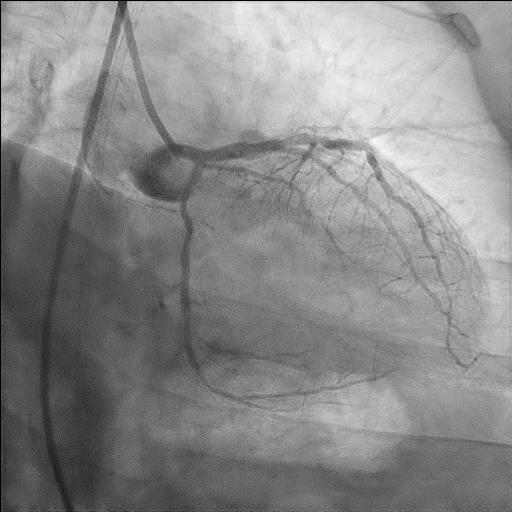
Diagnostic angiogram revealed mild plaque in both left anterior descending (LAD) and dominant right coronary artery (RCA). Target vessel for PCI was proximal LCx CTO with J-CTO score 3 (blunt stump, length > 20 mm, re-attempt) receiving Rentrop 3 collaterals from RCA. There was a ramus intermediate (RI) side branch that bifurcates immediately prior to proximal CTO cap. The LCx CTO was highly angulated from the left main (LM).

Interventional Management
Procedural Step
Vascular access via double puncture of bilateral femoral arteries with 7 Fr sheaths. XB 3.5 7 Fr (Cordis, U.S) engaged to LM while JR 4 7 Fr (Cordis, U.S) engaged to RCA for contralateral injection. SION blue (Asahi, Japan) wired to RI side branch and Crusade Type R microcatheter (Kaneka, Japan) advanced till ostial LCx bifurcation. Gladius EX 14 wire (Asahi, Japan) advanced via Crusade side port to attempt CTO puncture, but angle was unfavourable. Crusade exchanged to SuperCross 120 (Teleflex, U.S), providing better approach. Antegrade wire escalation with Gaia Next 1 (Asahi, Japan), ULTIMATEbros 3 (Asahi, Japan) and Gaia Next 2 was successful in crossing CTO. SuperCross 120 exchanged to Corsair (Asahi, Japan) via balloon trapping. Anchor balloon with Trek 2.0 x 12 mm (Abbott, U.S) deployed at RI to assist advancement of Corsair through CTO segment. CTO wire de-escalated to SION Blue. Sequential predilatation with Trek 1.5 x 12 mm and Trek 2.0 x 12 mm at 14 atm. IVUS (Boston, U.S) confirmed true lumen wiring with distal LCx vessel size 2.5 mm and proximal LCx 3.0 mm, minimal calcification. Further predilatation with NC Trek 2.5 x 15 mm at 12 atm, followed by deployment of SeQuent Please NEO 2.5 x 35 mm (B Braun, Germany) at 8 atm for 60 seconds at distal LCx. Proximal LCx prepared with Wolverine 3.0 x 15 mm (Boston, U.S) at 14 atm. Second SeQuent Please NEO 3.0 x 20 mm deployed at 10 atm for 60 seconds at proximal LCx. TIMI 3 flow achieved with minimal recoil and dissection.


Case Summary
This case highlights the successful use of an angulated microcatheter in directing wire position to guide puncture of the CTO cap of an angulated vessel. IVUS is useful to confirm true lumen wiring as well as determining lesion morphology and vessel size. The use of drug coated balloon strategy in this scenario simplifies an otherwise complex strategy of drug eluting stent deployment into the left main with potential carina shift compromising flow into the left main trifurcation.