
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-206
Saving the Day: Thrombus Showdown in the Right Coronary Artery
By Wei Juan Lim, Hoong Sheng Loh, Kumara Gurupparan Ganesan
Presenter
Wei Juan Lim
Authors
Wei Juan Lim1, Hoong Sheng Loh1, Kumara Gurupparan Ganesan1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-206
Endovascular - Thrombus Removal Devices and Techniques
Saving the Day: Thrombus Showdown in the Right Coronary Artery
Wei Juan Lim1, Hoong Sheng Loh1, Kumara Gurupparan Ganesan1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
31 years old gentleman with no known medical illness presented with typical angina to emergency department. The chest pain was left sided with radiation to jaw and arm, associated with shortness of breath. Blood pressure at arrival was 123/70mmHg with pulse rate of 79beats per minute. Other physical examinations were unremarkable.

Relevant Test Results Prior to Catheterization
Electrocardiogram showed sinusrhythm with T inversion at inferior leads. Full blood test and renal functionwere normal.
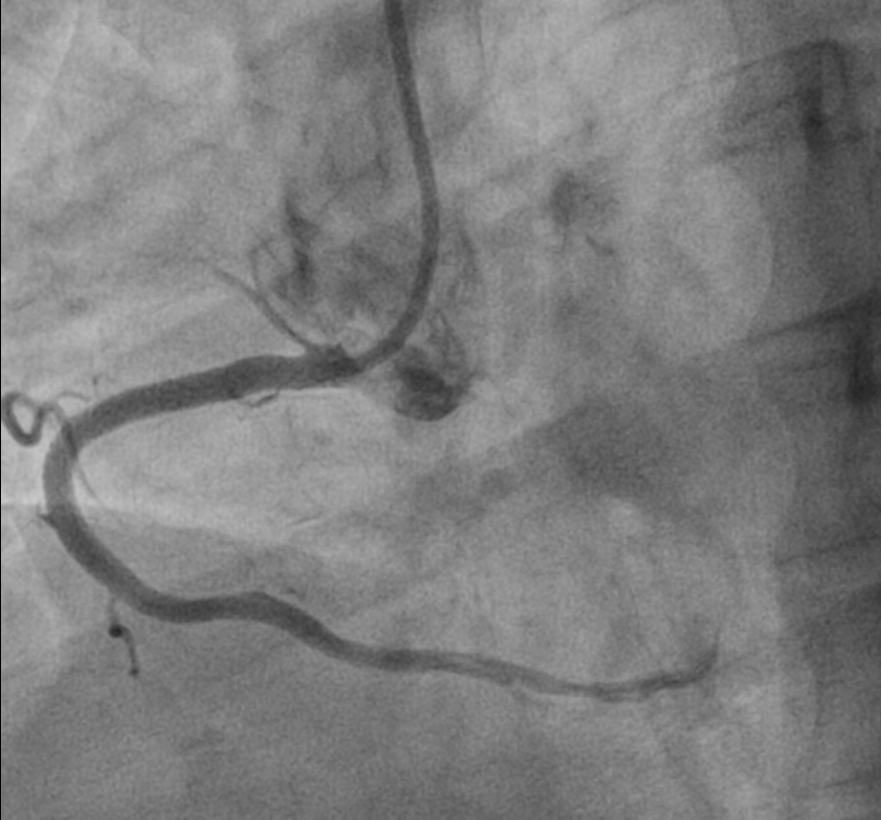
Relevant Catheterization Findings
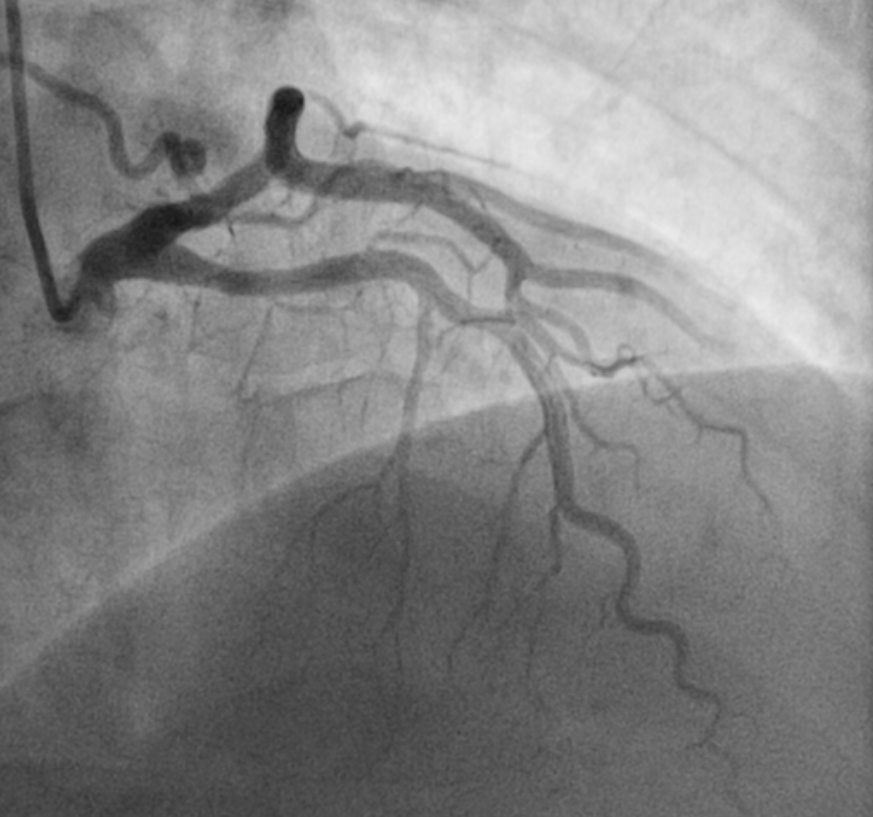
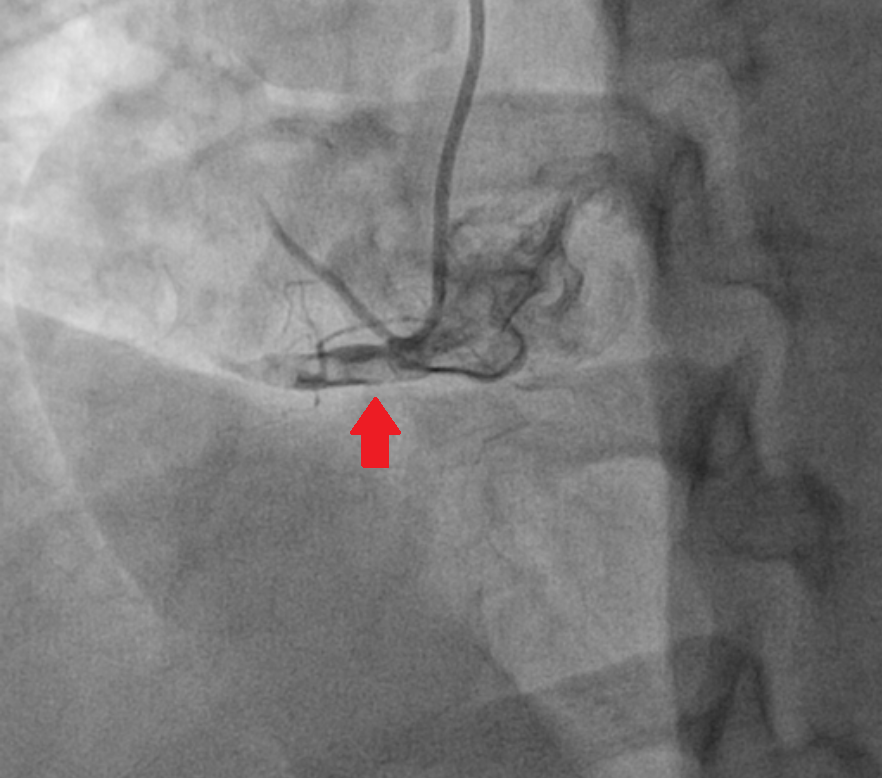
We proceeded with coronaryangiogram which showed normal left main stem with tortuous left circumflex,supplying retrograde flow to right coronary artery. Left anterior descendingartery has moderate lesion at proximal segment. Right coronary artery (RCA)showed acute on chronic total occlusion with heavy thrombus burden can be seenat proximal RCA.

Interventional Management
Procedural Step
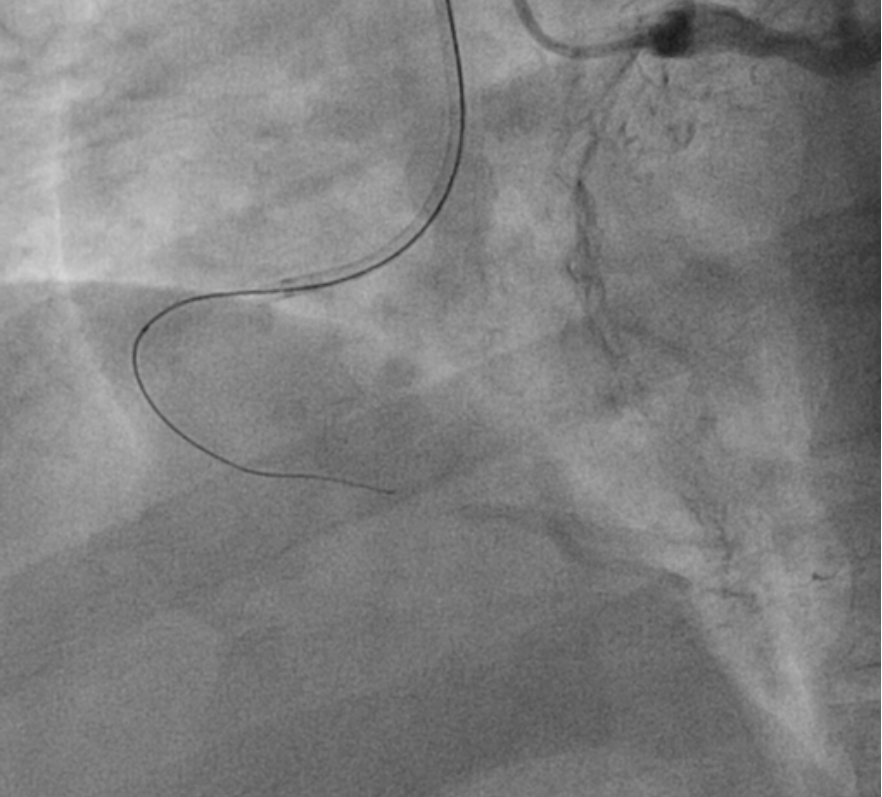
We have decided to proceed with coronary angioplasty of right coronary artery (RCA) in view of non-ST elevation myocardial infarction (NSTEMI). We used SAL 0.7 to engage RCA with side-holes at the catheter to prevent blood pressure dampening. We then wired down RCA with finecross microcatheter with fielder XT wire. We managed to wire down with the help of retrograde shot from left system.
We exchanged fielder XT wire with runthrough floppy wire using balloon trapping technique. In view of heavy thrombus burden at proximal RCA, we used export thrombus suction catheter to remove thrombus and also direct thrombus suction from the SAL catheter. Both showed heavy thrombus from the suction. We then gave intracoronary aggrastat to further lyse the thrombus.
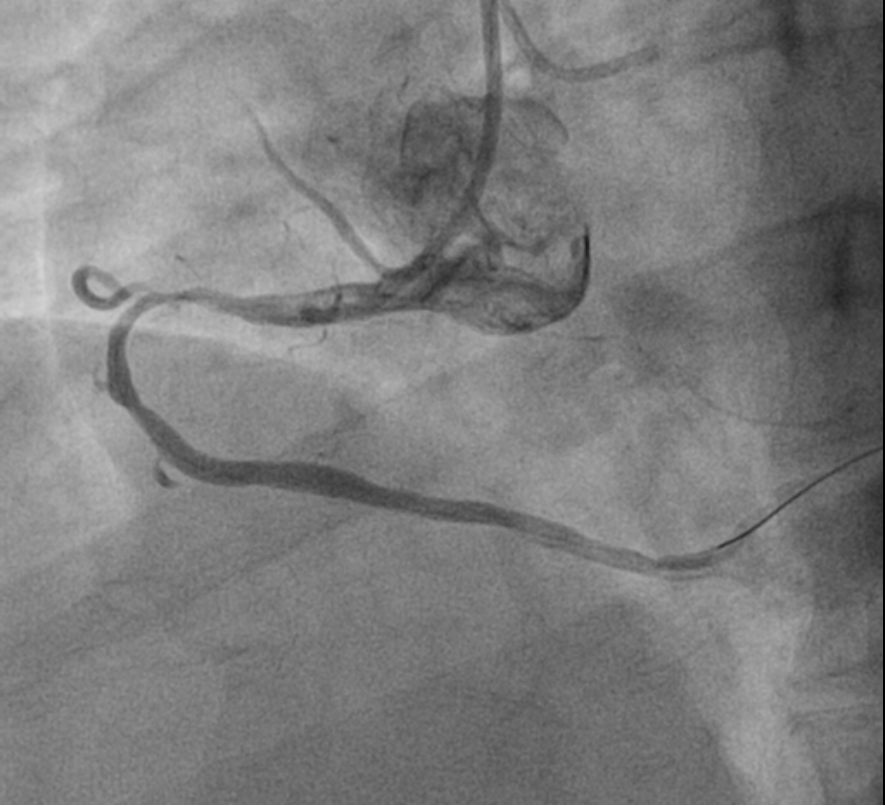
We then used Ryurei 2.0 x 15mmballoon to predilate and then further prepared the lesion with Wedge NC 3.0 x15mm up to 20 atmosphere. After adequate lesion preparation, we stented the proximal RCA with Resolute Onyx 3.5x38mm and post-dilated the stent with Apollo NC 3.75 x 15mm up to 22 atmosphere.
Post angioplasty showed TIMI 3flow with no dissection.
We exchanged fielder XT wire with runthrough floppy wire using balloon trapping technique. In view of heavy thrombus burden at proximal RCA, we used export thrombus suction catheter to remove thrombus and also direct thrombus suction from the SAL catheter. Both showed heavy thrombus from the suction. We then gave intracoronary aggrastat to further lyse the thrombus.
We then used Ryurei 2.0 x 15mmballoon to predilate and then further prepared the lesion with Wedge NC 3.0 x15mm up to 20 atmosphere. After adequate lesion preparation, we stented the proximal RCA with Resolute Onyx 3.5x38mm and post-dilated the stent with Apollo NC 3.75 x 15mm up to 22 atmosphere.
Post angioplasty showed TIMI 3flow with no dissection.
Case Summary
High thrombus burden duringangioplasty is a nightmare to all interventional cardiologist as the thrombusmight dislodge into main aorta and cause acute stroke. Appropriate thrombussuction with glycoprotein IIb/IIIa inhibitors infusion is one of the effectiveways. From a total occlusion with high thrombus burden to a TIMI 3 flow, wemanaged to open up the infarct related artery and relief chest pain for ourpatient.