
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-078
When It Seems Hopeful .. A Full Time Attempt Antegrade CTO
By Ramy Mohamed Atlm, Salma Mohamed Elshokafy
Presenter
Salma Elshokafy
Authors
Ramy Mohamed Atlm1, Salma Mohamed Elshokafy1
Affiliation
Tanta University Hospital, Egypt1,
View Study Report
TCTAP C-078
Coronary - Complex PCI - CTO
When It Seems Hopeful .. A Full Time Attempt Antegrade CTO
Ramy Mohamed Atlm1, Salma Mohamed Elshokafy1
Tanta University Hospital, Egypt1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
MaMal Male patient, aged 62 years old , Heavysmoker , not known to be Diabetic or Hypertensive, Dyslipidemic.( LDL 220 ) .
Cardiachistory of Ischemic heart disease one year ago with recurrent attacks of typical anginal pain refractory to medicaltreatment .
Generally : No signs or symptoms ofheart failure Local ex: Audible HS with no addedmurmurs
HR : 72
RBS : 145
Cardiachistory of Ischemic heart disease one year ago with recurrent attacks of typical anginal pain refractory to medicaltreatment .
Generally : No signs or symptoms ofheart failure Local ex: Audible HS with no addedmurmurs
HR : 72
RBS : 145
Relevant Test Results Prior to Catheterization
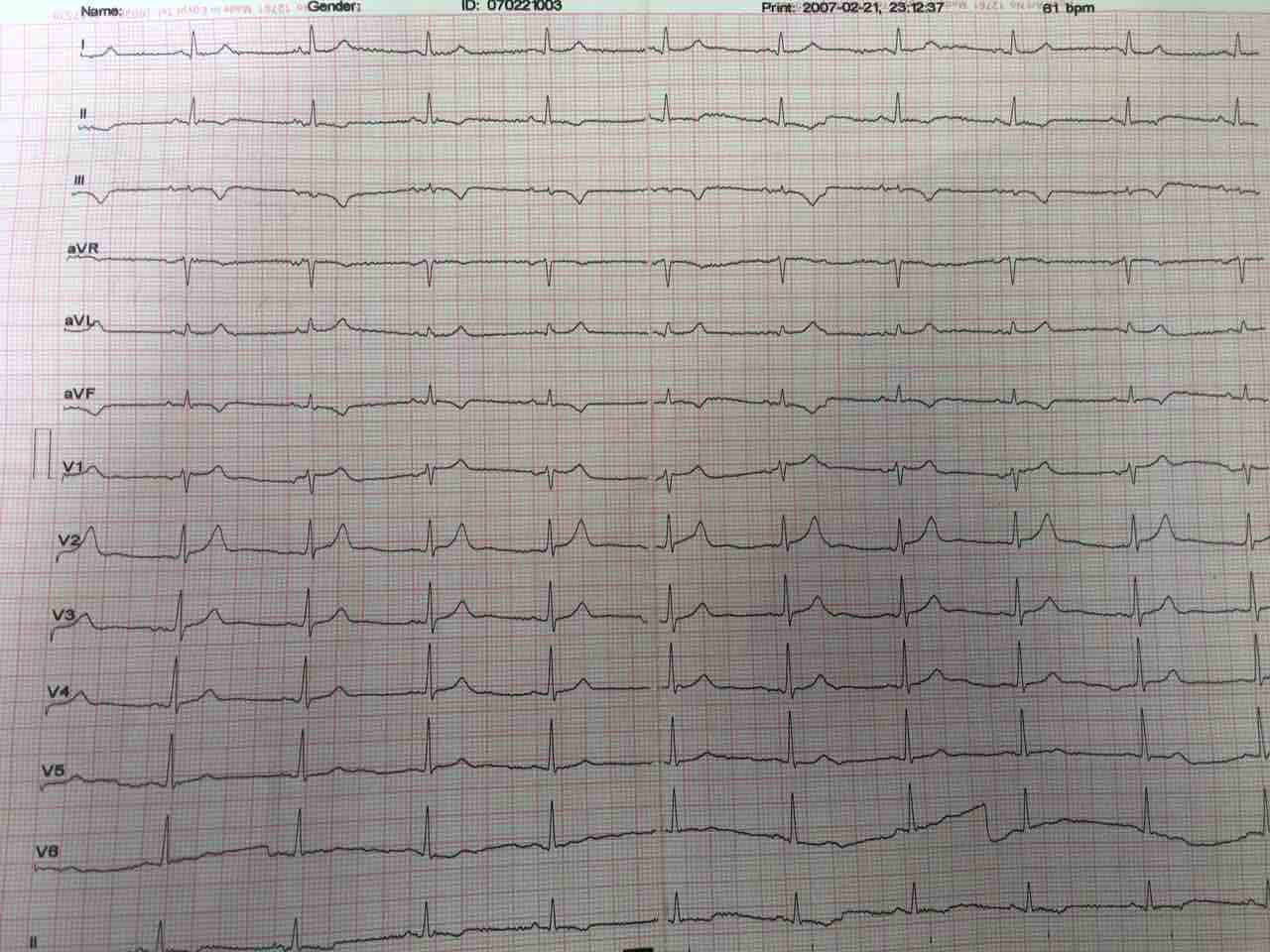
ECG: Normal sinus rhythm with ST Depression and T wave inversion in inferior leads
ECHO: Ischemic heart disease with average systolic function , RSWMAs in the form of (Apico-inferior , mid and basal inferior and infero-septal wall hypokinesia ) , with moderate mitral valve incompetence
ECHO: Ischemic heart disease with average systolic function , RSWMAs in the form of (Apico-inferior , mid and basal inferior and infero-septal wall hypokinesia ) , with moderate mitral valve incompetence
Relevant Catheterization Findings
LM : Normal vessel bifurcating into LAD and LCX.
LAD : Atherosclerotic vessel with no significant lesions .
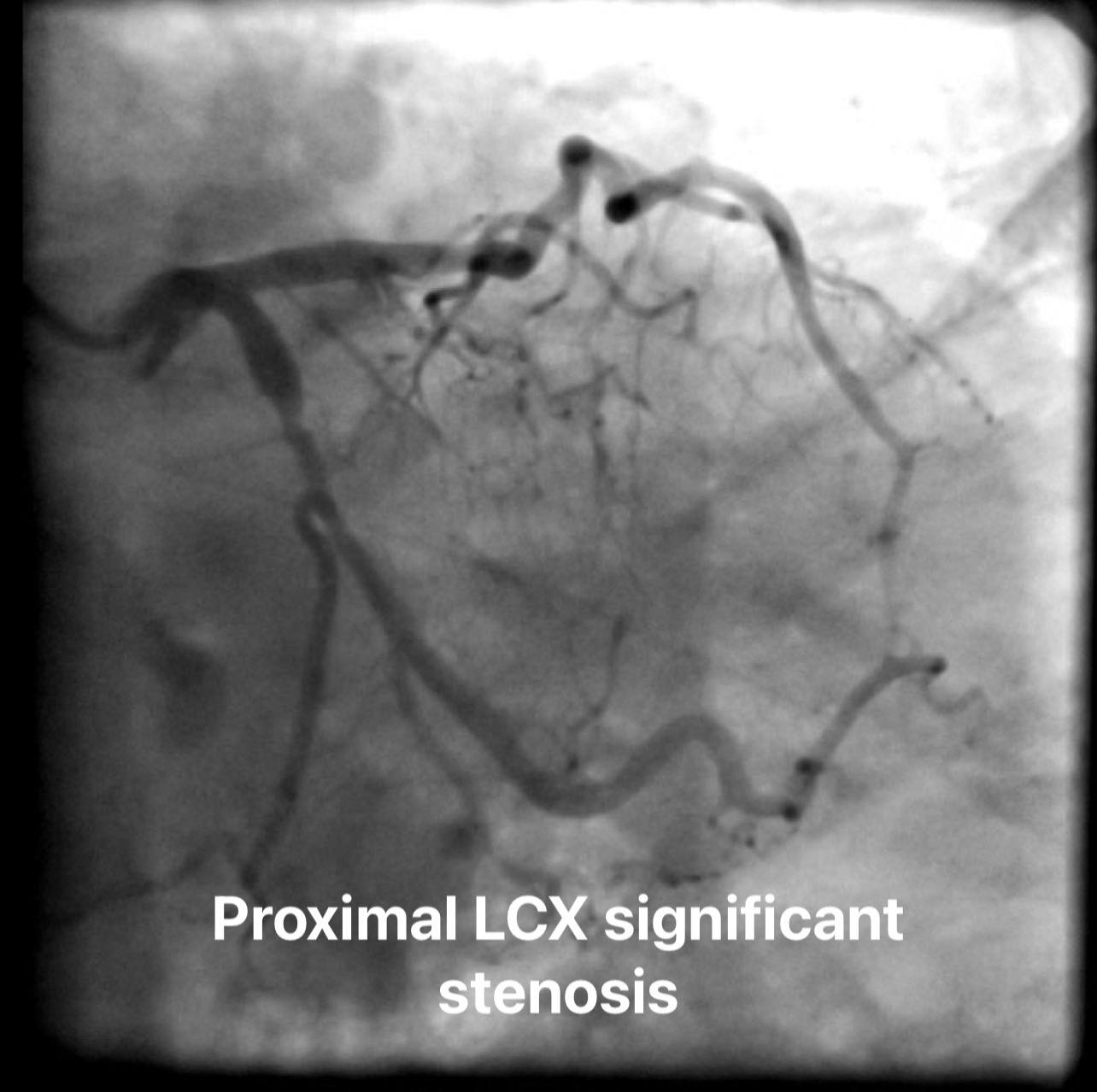
LCX : Atherosclerotic vessel with proximal significant stenosis .
RCA : Atherosclerotic vessel with long proximal to midsegmentchronic total occlusion receiving collaterals from left system
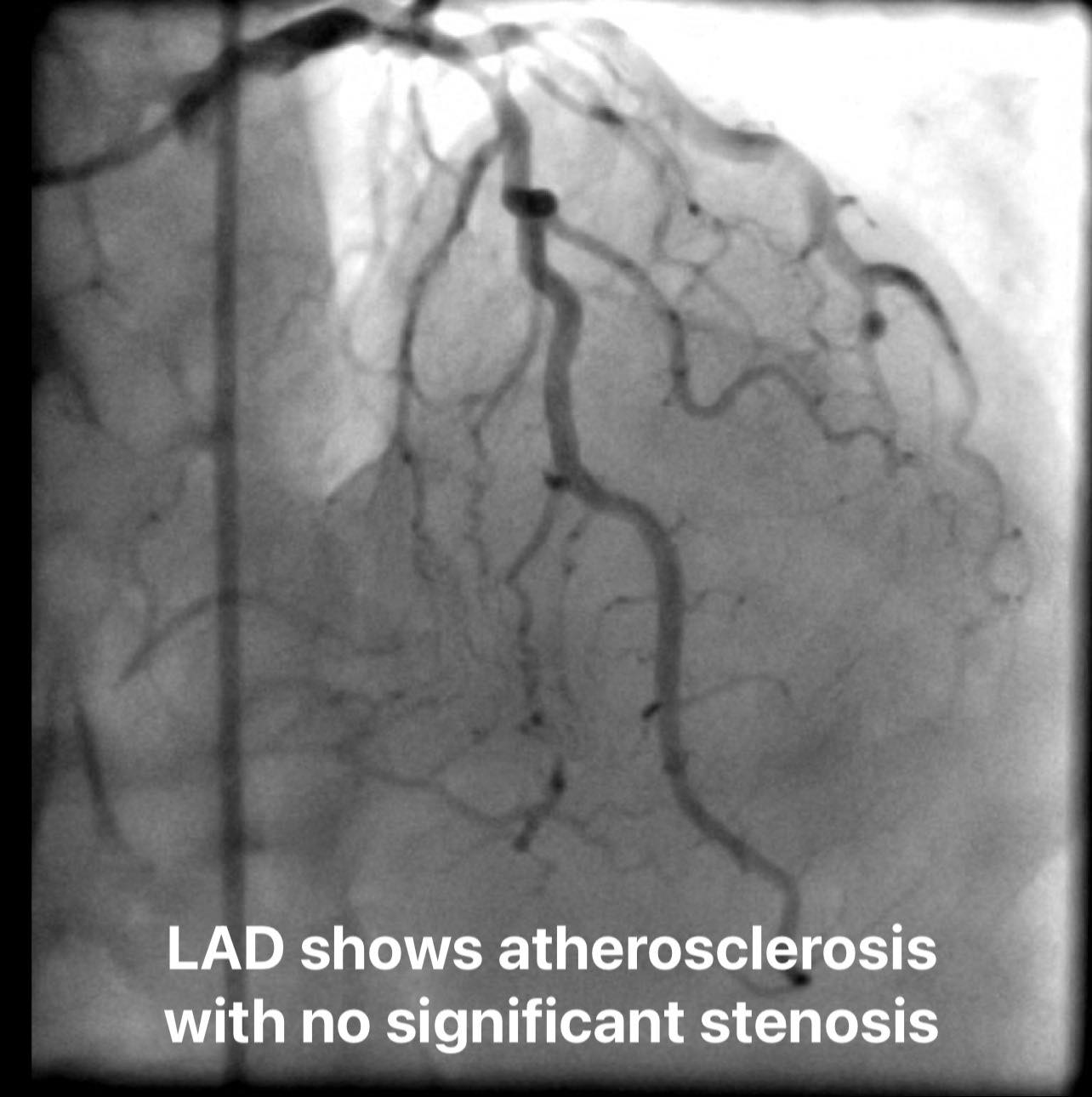

LAD : Atherosclerotic vessel with no significant lesions .
LCX : Atherosclerotic vessel with proximal significant stenosis .
RCA : Atherosclerotic vessel with long proximal to midsegmentchronic total occlusion receiving collaterals from left system
Interventional Management
Procedural Step
Our strategy was to go for PCI LCX which was done successfully with one DES , then trial PCI to CTO RCA antegradely first through( AWE or ADR ) and if failed we will try to go retrograde through septal collaterals.
But due to weak guiding support , we decided to balloon anchor in RV branch using BMW and 2.25*15 balloon together with power knuckle using inflated balloon 3x20 over pilot 50 and corsair MC over knuckled fielder XTA but also failed to cross , So we exchanged Fielder XTA with knuckled Fighter wire which succeeded to cross the CTO segment true lumen that was confirmed with dual injection that showed also big occluded PDA branch, So another Pilot50 wire was advanced to PDA through dual lumen MC Nhancer Rx with successful passage of wire into true lumen,then predilatation of PDA with 2.25 * 15balloon & Sequential predilatations to RCA was done by 2*20 ,, 2.25*20balloons with good distal run off , followed by stenting of RCA distally with3.5*38 DES & another 4*48 stent was deployed ostealy overlapping with the previous one and final post dilatation to the deployed stents with 4* 20 with good final result

But due to weak guiding support , we decided to balloon anchor in RV branch using BMW and 2.25*15 balloon together with power knuckle using inflated balloon 3x20 over pilot 50 and corsair MC over knuckled fielder XTA but also failed to cross , So we exchanged Fielder XTA with knuckled Fighter wire which succeeded to cross the CTO segment true lumen that was confirmed with dual injection that showed also big occluded PDA branch, So another Pilot50 wire was advanced to PDA through dual lumen MC Nhancer Rx with successful passage of wire into true lumen,then predilatation of PDA with 2.25 * 15balloon & Sequential predilatations to RCA was done by 2*20 ,, 2.25*20balloons with good distal run off , followed by stenting of RCA distally with3.5*38 DES & another 4*48 stent was deployed ostealy overlapping with the previous one and final post dilatation to the deployed stents with 4* 20 with good final result
Case Summary
Detailed understanding of angiogram and procedural planningis fundamental to successful CTO procedure and reduce difficulties through the procedure .