Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200925_013
| Complications - Complications | |
| Timely Intervention of Missed Catheter Induced Catastrophic Occlusive Dissection of LMCA | |
| Siddharth Bajaj1 | |
| Apollo Hospitals, India1, | |
|
[Clinical Information]
- Patient initials or identifier number:
P Anuradha
-Relevant clinical history and physical exam:
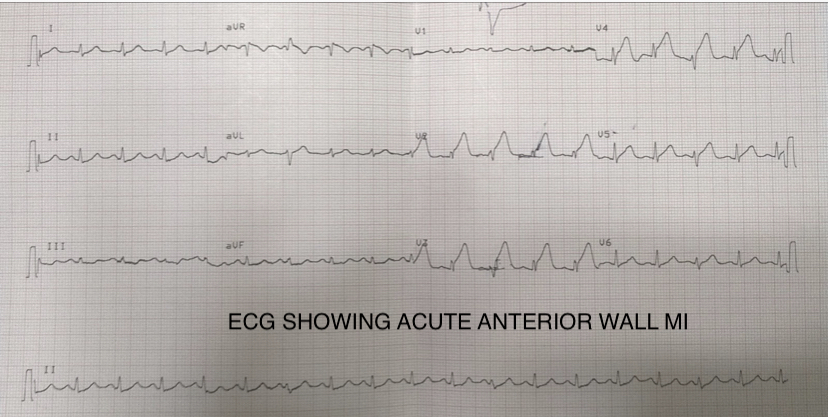
A 49-year-old woman diabetic, hypertensive , and hyperlipidemia presented to the emergency room at our center with sudden onset of severe chest pain of 2 hours duration around 5pm on 19th July 2020. Her ECG and 2D Echocardiogram were consistent with acute anterior wall myocardial infarction. She was given a loading dose of aspirin 325mg and ticagrelor 180 mg and was taken up for primary angioplasty.
 -Relevant test results prior to catheterization:
Coronary angiogram revealed 95% narrowing , an ulcerated plaque with grade 3 thrombus in the proximal LAD. Patient underwent Primary Percutaneous Transluminal Coronary Angioplasty (PTCA) and stenting with Xience Expedition 3.0 x 33mm stent to the proximal LAD.
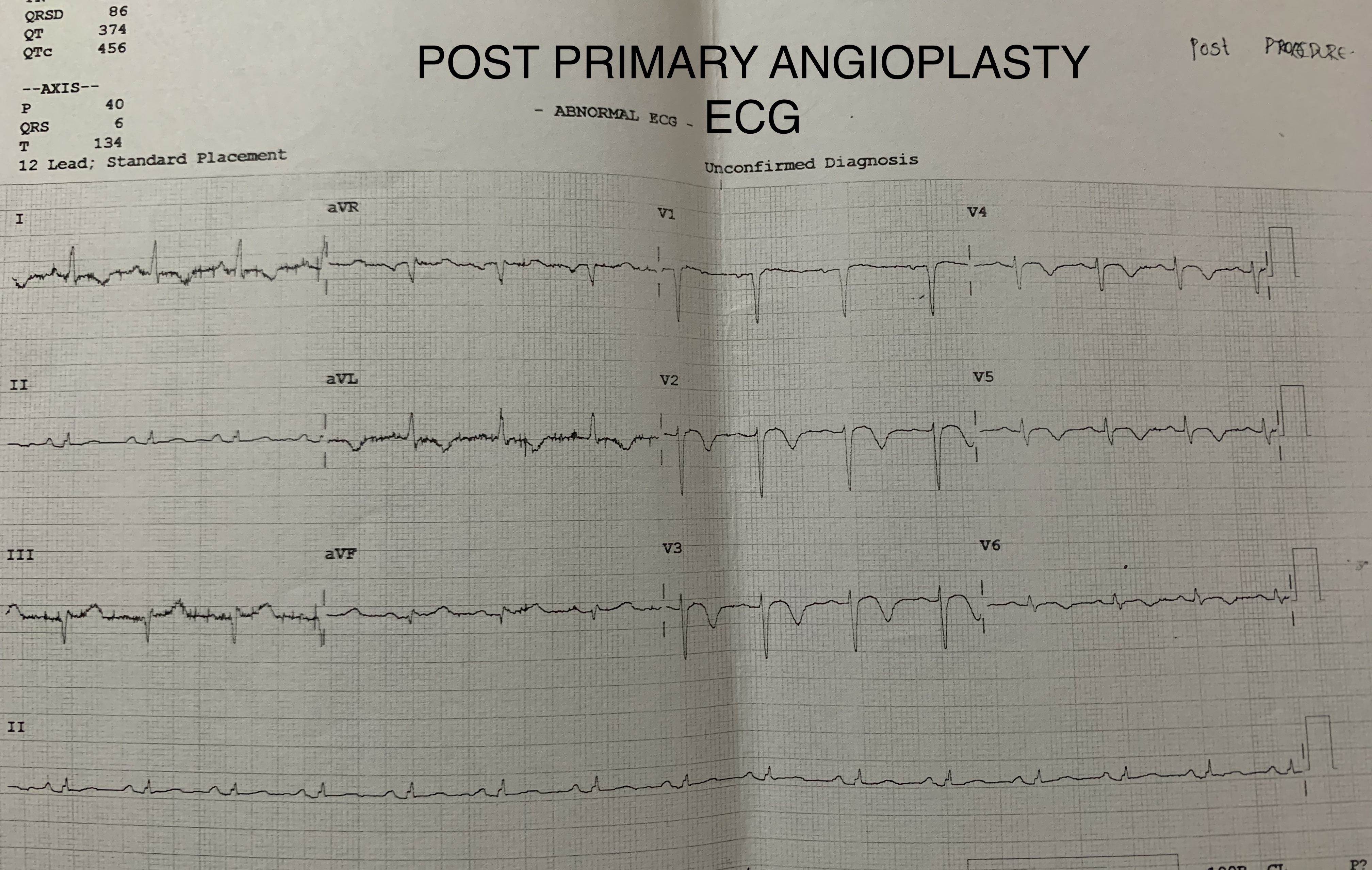  - Relevant catheterization findings:
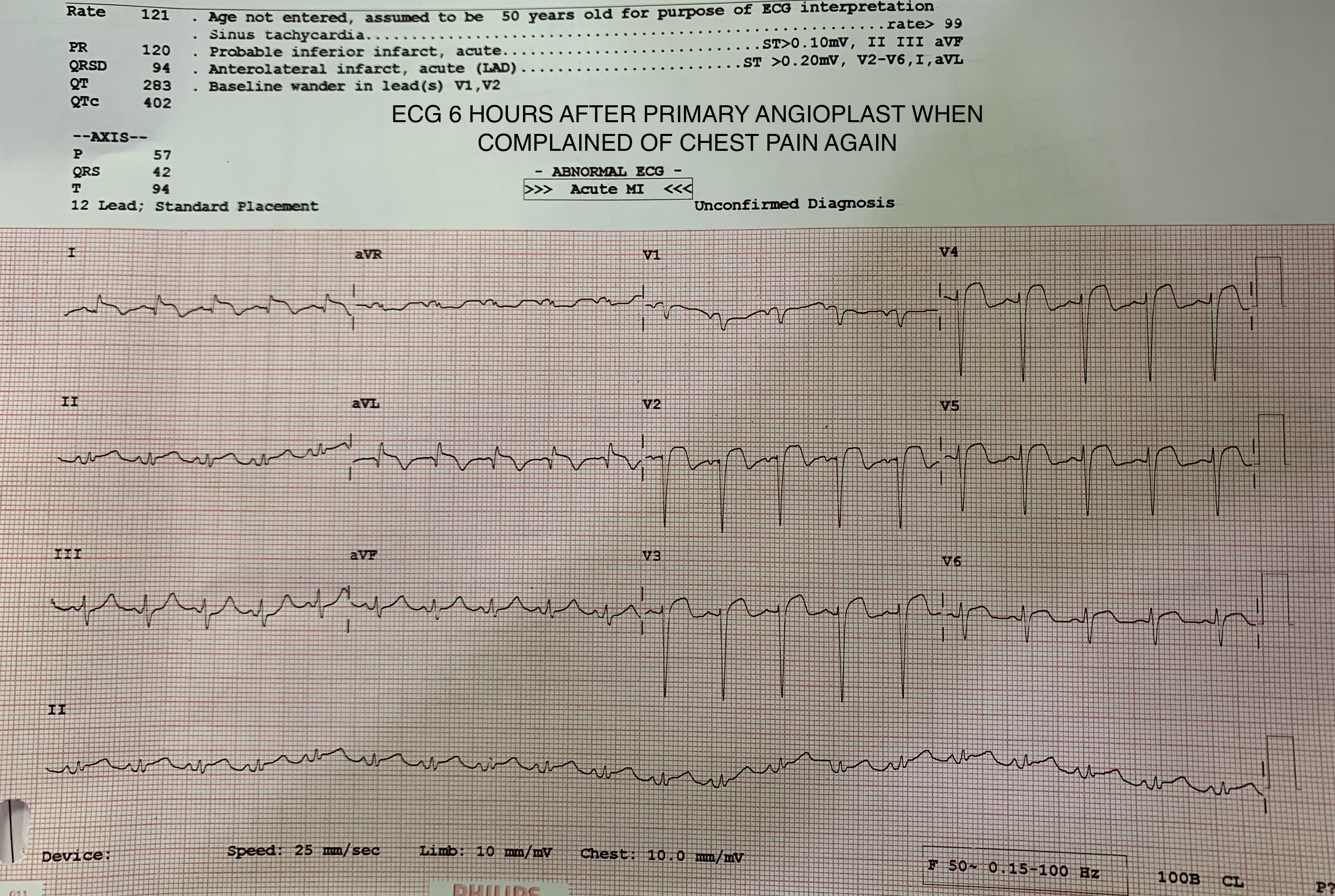
Final angiogram showed TIMI III flow with good result and ECG showed resolution of ST elevations. Patient was hemodynamically stable until 6 hours post procedure around 1am on 20th July 2020, when she developed anginal chest pain again with profuse sweating, ECG showed ST segment re-elevations in anterior leads. Check angio revealed acute stent thrombosis. Plain Old Balloon Angioplasty (POBA) was done with TIMI III flow with good result and patient was put on Gp IIb/IIIa inhibitor.
|
|
|
[Interventional Management]
- Procedural step:
6 hours after the POBA procedure , patient became hypotensive, had profuse sweating and chest discomfort and ECG revealed qRBBB . She was started on ionotropes and taken up immediately for Check Coronary Angiogram with IABP on Stand by. Her previous POBA procedure was quickly reviewed where a LMCA dissection flap was noticed in the RAO cranial view which was missed during the index procedure. The initial caudal view on check angiogram did not show any evidence of dissection and it appeared like LAD stent occlusion and LCX proximal occlusion. But the RAO Cranial view revealed a dissection in the LMCA extending to ostium of the LAD contained by the Stent in the proximal LAD with thrombus in the LAD and total occlusion of the proximal LCX with thrombus. Initial attempt was made to cross the lesion in the LMCA-LAD with a BMW wire but the wire entered the false lumen and it couldn't be passed into the LAD. After the true lumen was clearly identified, it was wired with a Whisper wire, which was also used to cross the lesion in the LMCA-LAD. Initially a hydrophilic wire was not chosen to cross the lesion in order to prevent extension of the dissection. Stenting was done by the Minicrush method as the LCX was the non-infarct related artery and hence was stented first. Simultaneous Kissing balloon inflation was performed and Re-POT was done. Final angiogram showed TIMI III flow in LMCA-LAD and LCX. Patient qRBBB resolved and the patient was shifted to the ICU on ionotropic support.
- Case Summary:
Guide induced coronary artery dissection can potentially cause devastating complications with favourable outcomes when recognised timely and treated with immediate stenting. Successful advancement of guide wires first into the true lumen of the LMCA, then into the true lumina of the LAD and LCX can be technically challenging, with unstable hemodynamics. When a dissection involves both the major branches, minicrush technique can be a preferred strategy in a hemodynamically unstable patient. This case highlights that doing a primary PCI procedure, even at odd hours in the night, all views must be reviewed at the end of the procedure, as a dissection flap may be missed in certain views.
|
|